UK Healthcare Settings and Professional Roles for Advance Decisions
Setting or professional | Typical relevance to an Advance Decision | Common practical actions | Relevant records or systems | Typical level of involvement | Key note |
|---|---|---|---|---|---|
Primary care | |||||
GP practice | Often the first place where an Advance Decision is discussed, recorded or reviewed. | Ask whether one exists, add alerts, code the record, and encourage clinical review. | GP electronic record, summary care information, care plan, ReSPECT or DNACPR records. | Usually central | GP records can help other services know the document exists, but clinicians must still consider validity and applicability. |
General practitioner | May explain medical consequences and document discussions about future treatment refusal. | Discuss treatment scenarios, assess capacity if relevant, update records, and signpost specialist advice. | Consultation notes, problem codes, care plans, medication records and referral letters. | Usually central | A GP cannot make the decision for the person but can help ensure it is clinically clear. |
Practice nurse | May become aware of future care wishes during long-term condition or frailty reviews. | Prompt discussion with a GP, note patient statements, and check whether records are up to date. | Long-term condition templates, care plans, GP record alerts and consultation notes. | Sometimes relevant | Nursing notes may prompt review, but treatment refusal decisions require validity and applicability checks. |
Emergency care | |||||
Out-of-hours GP service | May need to make urgent treatment decisions when the usual GP practice is closed. | Check shared records, ask attending carers or clinicians about documented refusals, and document decisions. | Out-of-hours clinical record, GP shared record, urgent care plan and ReSPECT form. | Often relevant | Urgency does not remove the need to consider any known Advance Decision that appears valid and applicable. |
NHS 111 | May identify that urgent care advice should take account of existing care planning documents. | Record caller information, escalate to clinicians, and direct urgent services to relevant care records. | 111 call record, clinical assessment system, urgent care plan and referral notes. | Sometimes relevant | Telephone triage may flag the issue, but treating clinicians decide after checking validity and applicability. |
Ambulance service | May encounter the document during collapse, serious illness or end-of-life emergencies. | Look for recorded care plans, consult clinical support, document findings and follow emergency protocols. | Electronic patient report form, shared care plan, ReSPECT form and DNACPR documentation. | Often relevant | Paramedics may need rapid decisions but must consider a known refusal if it is valid and applicable. |
Paramedic | May be the first clinician deciding whether to start, continue or withhold emergency treatment. | Assess capacity where possible, review available documents, seek senior advice and record rationale. | Ambulance clinical record, emergency care plan, ReSPECT form, DNACPR form and hospital handover notes. | Often relevant | If life-sustaining treatment is refused, statutory formalities are especially important. |
Emergency department | May need to decide quickly about resuscitation, ventilation, surgery, transfusion or admission. | Search hospital records, review ambulance handover, contact senior clinicians and document the decision. | Emergency department notes, EPR alerts, ambulance handover, ReSPECT form and DNACPR record. | Usually central | Emergency treatment can be affected only if the refusal is known, valid and applicable to the proposed treatment. |
Hospital care | |||||
Acute medical or surgical admissions unit | Admission clerking may reveal existing refusals relevant to investigations or treatment escalation. | Ask on admission, reconcile documents, add EPR alerts and involve senior decision-makers. | Admission clerking, hospital EPR, treatment escalation plan, ReSPECT form and discharge summary. | Often relevant | Hospital teams should not rely solely on admission labels applicability must be assessed against the specific treatment. |
Hospital ward team | May manage ongoing treatment decisions after admission when capacity changes. | Review notes, discuss with senior doctors, record capacity assessments and update care plans. | Ward notes, EPR alerts, capacity assessments, escalation plans and discharge summaries. | Often relevant | A refusal may apply later in the admission if the person loses capacity and the circumstances match. |
Specialist care | |||||
Intensive care unit | Commonly involves life-sustaining treatments that may be expressly refused. | Check for written refusal, confirm formalities, involve consultants and document best available evidence. | ICU notes, EPR, treatment escalation plan, ReSPECT form and critical care handover. | Usually central | Refusal of life-sustaining treatment must be written, signed, witnessed and state it applies even if life is at risk. |
Anaesthetist | May need to consider refusals affecting ventilation, resuscitation, blood products or perioperative escalation. | Review consent and capacity, check documents before procedures, and agree perioperative plans. | Anaesthetic chart, consent form, theatre checklist, EPR alerts and treatment escalation plan. | Sometimes relevant | Advance refusals should be checked before elective procedures where foreseeable treatments may be refused. |
Hospital care | |||||
Surgeon | May encounter refusals of surgery, transfusion, resuscitation or postoperative intensive care. | Clarify treatment scope, document consent discussions, and align escalation plans with any valid refusal. | Consent form, operation notes, EPR, blood refusal forms and escalation plan. | Sometimes relevant | A valid and applicable refusal can affect surgical treatment even where clinicians consider treatment beneficial. |
Specialist care | |||||
Oncology service | May discuss future refusal of chemotherapy, hospital admission, ventilation or other escalation. | Record treatment preferences, coordinate with palliative care and update care planning documents. | Oncology notes, chemotherapy plan, EPR, palliative care plan and clinic letters. | Often relevant | Future refusals should identify treatments and circumstances clearly enough to assess applicability. |
Renal dialysis service | May involve future refusal of dialysis or decisions about stopping dialysis if capacity is lost. | Document dialysis-specific wishes, involve consultants, and share plans with community and hospital teams. | Renal unit record, dialysis prescription, clinic letters, care plan and EPR alerts. | Often relevant | Treatment-specific wording is important where ongoing life-sustaining treatment may be refused. |
Cardiology service | May consider refusals relating to resuscitation, ventilation, device therapy or intensive care. | Review escalation preferences, record device-related discussions and coordinate with GP or palliative care. | Cardiology clinic letters, device records, EPR, ReSPECT form and escalation plan. | Sometimes relevant | Clinical plans should distinguish preferences from legally binding advance refusals. |
Respiratory service | May encounter refusals of non-invasive ventilation, intubation, ICU admission or antibiotics. | Record specific treatment refusals, update exacerbation plans and share with urgent care services. | Respiratory notes, COPD plan, oxygen records, EPR, ReSPECT form and discharge summary. | Often relevant | Applicability depends on the treatment refused and the clinical circumstances at the time. |
Neurology service | May support planning for progressive conditions affecting speech, swallowing, breathing or capacity. | Discuss future scenarios early, record refusals clearly, and coordinate with community teams. | Neurology letters, care plans, communication assessments, EPR and respiratory support plans. | Often relevant | Early documentation can be important before communication or decision-making capacity becomes impaired. |
Memory clinic or dementia service | May discuss future treatment refusals soon after diagnosis while the person has capacity. | Encourage timely planning, record capacity discussions and signpost legal or clinical advice. | Memory clinic letters, dementia care plan, GP record, EPR and capacity assessments. | Often relevant | An Advance Decision must be made while the person has capacity for the decision. |
Mental health service | May encounter treatment refusals, crisis plans and capacity issues during psychiatric care. | Check capacity, distinguish advance statements from refusals, and consider Mental Health Act issues. | Mental health record, crisis plan, care programme approach plan and hospital EPR. | Sometimes relevant | Advance Decisions interact with mental health law specialist legal and clinical review may be needed. |
Psychiatrist | May assess capacity and consider refusals of treatment during mental disorder or physical illness. | Assess decision-specific capacity, document reasoning and liaise with medical or legal teams. | Mental health notes, capacity assessments, risk plans, crisis plans and EPR. | Sometimes relevant | Capacity is decision-specific and time-specific under the Mental Capacity Act framework. |
Palliative care team | Frequently supports planning around treatments a person would refuse near end of life. | Clarify wishes, update care plans, coordinate records and discuss ReSPECT or DNACPR where appropriate. | Palliative care notes, EPaCCS, ReSPECT form, DNACPR form and hospice records. | Usually central | Care planning documents support access to information but do not replace the legal validity test. |
Hospice | May hold detailed end-of-life care discussions and coordinate treatment refusal information. | Review documents on admission, add care plan alerts and communicate with GP and hospital teams. | Hospice record, palliative care plan, EPaCCS, ReSPECT form and discharge or transfer notes. | Usually central | Hospice records should help clinicians identify the relevant refusal quickly during transfers or deterioration. |
Community care | |||||
Community nursing team | May notice changing health and help ensure advance care records are current and visible. | Ask about documents, update nursing notes, alert GP or palliative care team and record concerns. | Community nursing record, GP shared record, care plan, EPaCCS and ReSPECT form. | Often relevant | Community notes can be crucial for visibility, but clinicians must check legal status before relying on the refusal. |
District nurse | Often involved with frailty, long-term conditions and end-of-life care at home. | Check care plan location in records, communicate changes and prompt medical review if unclear. | District nursing notes, GP record, EPaCCS, ReSPECT form and medication administration records. | Often relevant | If circumstances change, the Advance Decision may need clinical review for continued applicability. |
Care home | |||||
Care home | May need to make sure staff and visiting clinicians know about relevant treatment refusals. | Record existence in care plans, alert visiting clinicians and ensure transfer information is accurate. | Care home care plan, medication records, GP record, transfer form, ReSPECT and DNACPR forms. | Often relevant | Care home staff usually support information sharing clinical decisions still require validity and applicability assessment. |
Care home nurse | May identify deterioration and communicate advance refusal information to GPs or emergency services. | Check care plan entries, contact GP or ambulance clinicians, and record handover information. | Nursing notes, care plan, medication administration record, ReSPECT form and transfer documentation. | Often relevant | Accurate handover can determine whether urgent clinicians see the refusal in time. |
Community care | |||||
Home care provider | May be aware of care preferences but is rarely responsible for treatment decisions. | Record relevant alerts, follow care plan instructions and notify clinical services if health changes. | Home care plan, visit notes, risk assessments and shared care communications. | Sometimes relevant | Care workers should escalate clinical questions rather than interpret legal validity themselves. |
Adult social worker | May encounter Advance Decisions during care assessments, safeguarding or capacity-related planning. | Record existence, share relevant information lawfully and involve health professionals for clinical questions. | Adult social care record, care and support plan, safeguarding records and MCA assessments. | Sometimes relevant | Social care records may support visibility but do not determine medical applicability of the refusal. |
Occupational therapist | May identify capacity, communication or home safety issues that prompt wider care planning. | Record relevant observations, raise concerns with clinicians and include alerts in care planning notes. | OT assessment, rehabilitation notes, care plan and shared community record. | Rarely directly involved | OT involvement is usually supportive rather than determinative for Advance Decision validity. |
Physiotherapist | May encounter care planning issues during rehabilitation after serious illness or hospital discharge. | Note relevant information, follow escalation plans and refer clinical legal questions to treating clinicians. | Physiotherapy notes, rehabilitation plan, discharge summary and shared care record. | Rarely directly involved | Rehabilitation goals should be distinguished from advance refusals of medical treatment. |
Specialist care | |||||
Speech and language therapist | May assist communication where a person is discussing or reviewing treatment refusals. | Assess communication needs, support accessible discussion and record communication aids used. | Communication assessment, swallowing plan, capacity assessment notes and shared care record. | Sometimes relevant | Supported communication may be important when assessing whether the person can make or confirm a decision. |
Administrative or records role | |||||
Hospital discharge team | May help transfer care planning information from hospital to GP, community services or care homes. | Include alerts in discharge documents, check care plan updates and communicate with receiving services. | Discharge summary, EPR, transfer of care document, ReSPECT form and community referral records. | Sometimes relevant | Poor discharge communication can make a valid refusal hard to identify in later urgent care. |
Hospital medical records department | May scan, index or flag documents so clinicians can find them when needed. | Upload documents accurately, use correct document type and maintain clear record alerts. | Hospital EPR, scanned document repository, patient administration system and clinical alerts. | Sometimes relevant | Records staff support access clinicians remain responsible for legal and clinical assessment. |
GP reception or administration team | May receive documents and route them for coding or clinical review. | Scan documents, notify clinical staff and avoid giving legal or clinical interpretation. | GP document workflow, coded record, alerts, tasks and correspondence log. | Sometimes relevant | Administrative handling should trigger clinician review where the document may affect treatment. |
Clinical coding or records coding team | May code the existence of relevant advance care planning documents in electronic records. | Use accurate codes, avoid misleading labels and ensure scanned documents are linked where possible. | SNOMED CT codes, GP record, hospital EPR, clinical alerts and document management systems. | Rarely directly involved | Coding indicates possible existence it is not proof that the refusal is valid or applicable. |
Shared care record service | May allow different NHS and care services to see relevant care planning information. | Maintain visibility of alerts, support lawful information sharing and avoid duplicate inconsistent entries. | Shared care record, GP record extracts, hospital EPR feeds and community care records. | Sometimes relevant | Shared records improve discoverability, but the underlying document and current circumstances must still be assessed. |
Electronic Palliative Care Coordination System | May record key end-of-life preferences and alert services to treatment refusal documents. | Update care plan entries, record document existence and share with urgent and community services. | EPaCCS, palliative care record, GP record, ambulance access record and ReSPECT form. | Often relevant | EPaCCS entries help coordination but should not be treated as a substitute for statutory requirements. |
Hospital care, Emergency care, Community care, Care home | |||||
ReSPECT process | Creates personalised emergency care recommendations that may refer to an Advance Decision. | Record recommendations, note legal documents, review after major changes and share across settings. | ReSPECT form, emergency care plan, GP record, hospital EPR and ambulance records. | Often relevant | ReSPECT is a clinical process a valid and applicable Advance Decision has separate legal effect. |
DNACPR decision process | May overlap where an Advance Decision refuses CPR in specified circumstances. | Check whether CPR refusal is in an Advance Decision, ReSPECT form or DNACPR record. | DNACPR form, ReSPECT form, GP record, hospital EPR and ambulance record. | Often relevant | DNACPR records and Advance Decisions are distinct clinicians must identify which document they are relying on. |
Hospital care | |||||
Clinical ethics committee | May advise where there is uncertainty or disagreement about treatment refusal. | Review facts, advise clinicians, document ethical reasoning and suggest legal advice if needed. | Ethics referral, meeting note, hospital EPR, legal advice record and capacity assessments. | Rarely directly involved | Ethics advice does not replace the statutory test for validity and applicability. |
Administrative or records role | |||||
NHS trust legal services | May advise clinicians on disputes, uncertainty or court applications involving treatment refusal. | Review documents, advise on legal risk and coordinate urgent Court of Protection input if required. | Legal advice file, EPR note, capacity evidence, ethics notes and court documents. | Rarely directly involved | Serious disputes may require urgent legal advice or Court of Protection involvement. |
Court of Protection proceedings | May determine disputes about capacity, validity, applicability or serious medical treatment. | Preserve evidence, obtain legal advice and seek urgent directions where treatment decisions cannot wait. | Court application, witness evidence, medical records, capacity assessments and orders. | Rarely directly involved | Court involvement is usually reserved for serious uncertainty or disagreement, not routine recording. |
Community care, Hospital care | |||||
Independent Mental Capacity Advocate | May be involved in serious medical treatment decisions for certain people who lack capacity and support. | Gather views, review records, represent the person and raise any known treatment refusals. | IMCA report, capacity assessment, best interests records and medical notes. | Sometimes relevant | IMCA involvement does not override a valid and applicable Advance Decision. |
Primary care, Hospital care, Community care | |||||
Hospital or community pharmacist | May notice medication refusals or care plan alerts during medicines review or dispensing. | Record medication-related concerns, alert prescribers and avoid interpreting broader treatment refusals alone. | Medication record, discharge medicines service record, pharmacy notes and GP or hospital EPR. | Rarely directly involved | Medication preferences should be distinguished from a legally effective refusal of specified treatment. |
Specialist care | |||||
Blood transfusion team | May need to identify and respect a clear advance refusal of blood or blood products. | Check refusal documentation, inform surgical and anaesthetic teams, and document alternatives discussed. | Transfusion record, consent form, EPR alert, blood refusal form and operation notes. | Sometimes relevant | Specificity matters because clinicians must know which products and circumstances are refused. |
Maternity service | May encounter refusals relevant to obstetric surgery, transfusion or emergency treatment. | Discuss foreseeable emergencies, document treatment refusals and involve obstetric anaesthetic specialists. | Maternity notes, birth plan, consent records, EPR alerts and transfusion documentation. | Rarely directly involved | Advance refusals should be considered against the exact treatment and emergency circumstances. |
Learning disability liaison team | May support communication, reasonable adjustments and capacity assessment in hospital or community care. | Identify communication needs, support decision-making and alert clinicians to existing documents. | Hospital passport, reasonable adjustment flag, capacity assessment, care plan and EPR. | Sometimes relevant | A person must be supported to make decisions before being treated as lacking capacity. |
Hospital care, Emergency care | |||||
Emergency theatre team | May need to act quickly where surgery, anaesthesia, transfusion or resuscitation is refused. | Check EPR alerts, review consent and escalation plans, and involve senior surgical and anaesthetic staff. | Theatre checklist, consent records, anaesthetic chart, EPR alerts and transfusion documentation. | Sometimes relevant | Emergency context increases urgency but does not nullify a known valid and applicable refusal. |
Hospital care, Community care | |||||
Inpatient rehabilitation unit | May review future care plans after stroke, brain injury or major illness. | Record capacity recovery, review previous refusals and update discharge care planning information. | Rehabilitation notes, capacity assessments, discharge summary, care plan and EPR. | Sometimes relevant | If the person regains capacity, current decisions usually take priority over earlier planning records. |
Primary care, Community care | |||||
Prison healthcare service | May need to record advance refusals for people receiving healthcare in custody. | Add health record alerts, coordinate with hospitals and ensure urgent transfer information is accurate. | Prison healthcare record, GP-equivalent record, hospital referral letters and transfer documentation. | Rarely directly involved | Custody does not remove the need to consider capacity and any valid applicable refusal. |
Hospital care, Specialist care | |||||
Private hospital or independent clinic | May need to check advance refusals before procedures, admissions or transfers to NHS care. | Ask pre-admission questions, record alerts, review consent and include information in transfer letters. | Independent provider record, consent form, theatre records, transfer letter and EPR alerts. | Sometimes relevant | The Mental Capacity Act framework applies to private healthcare as well as NHS treatment decisions. |
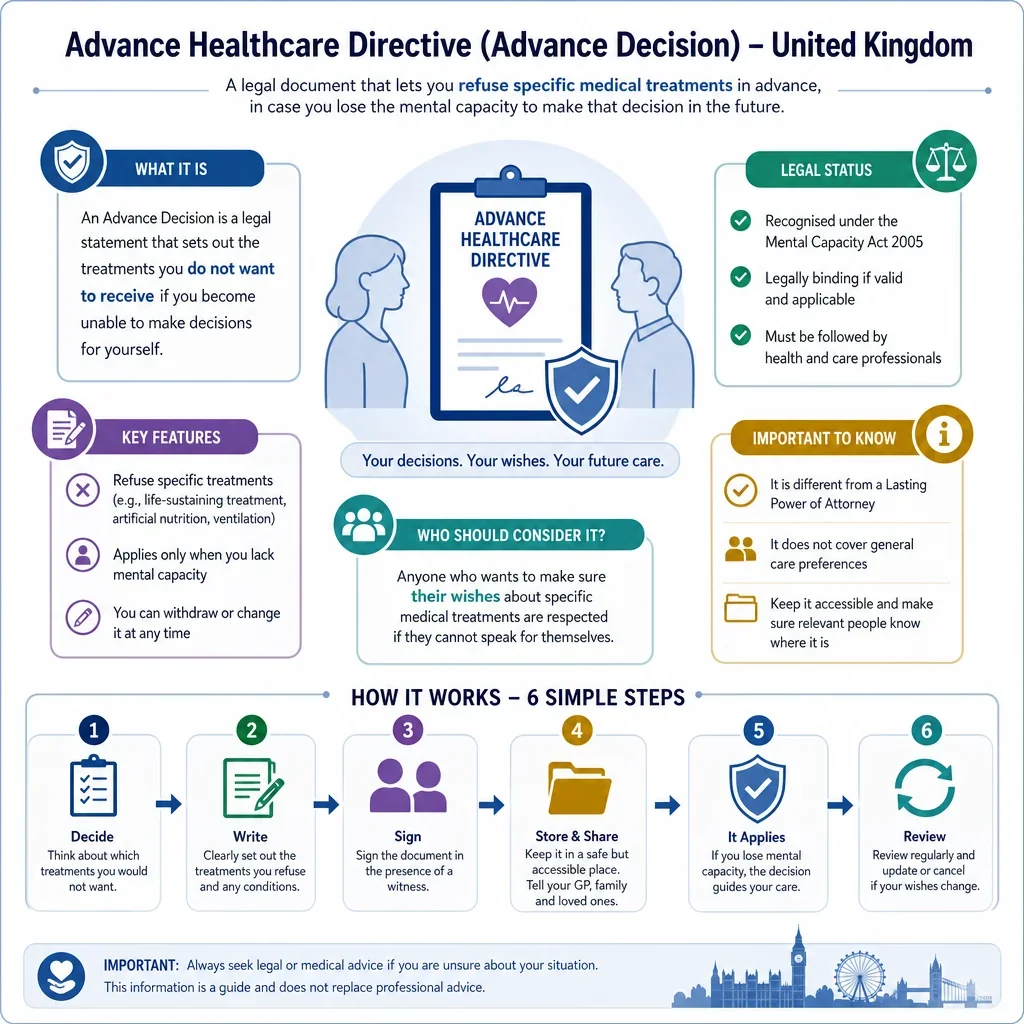
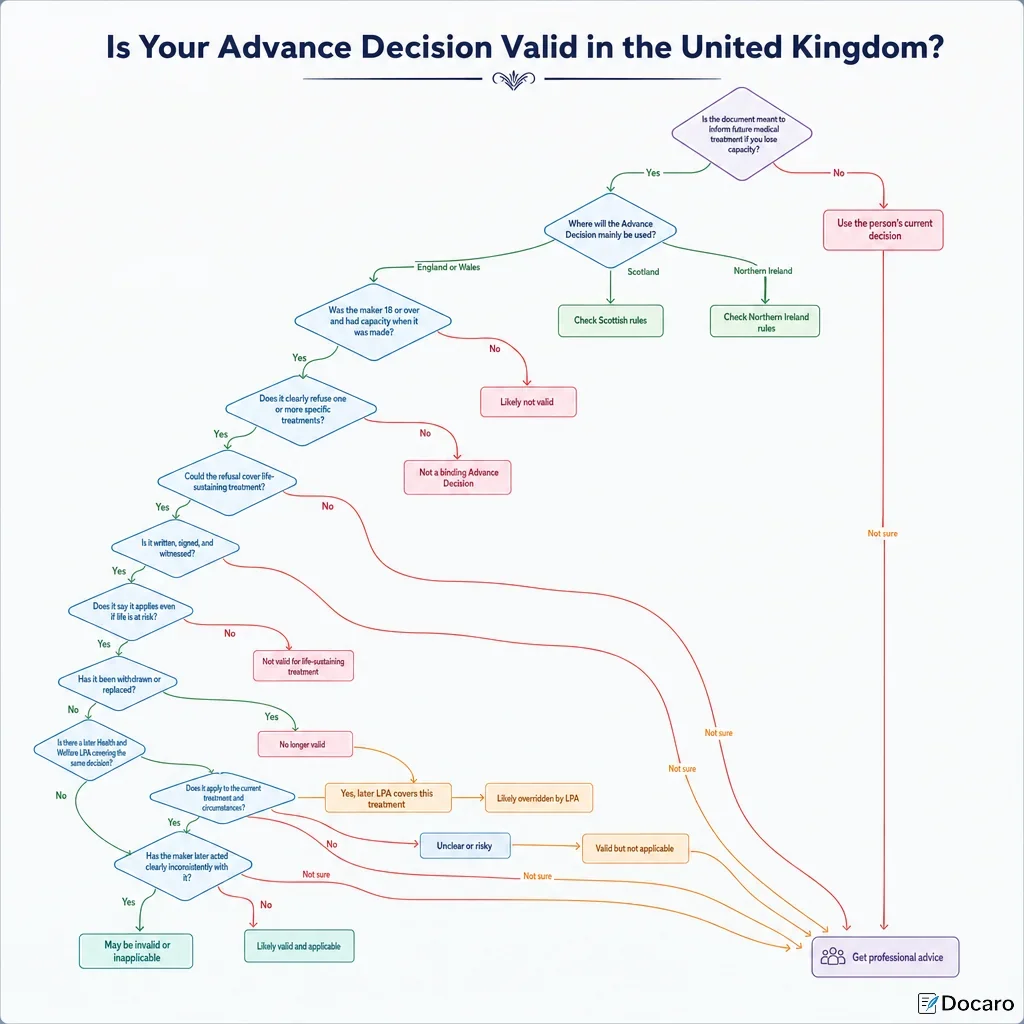
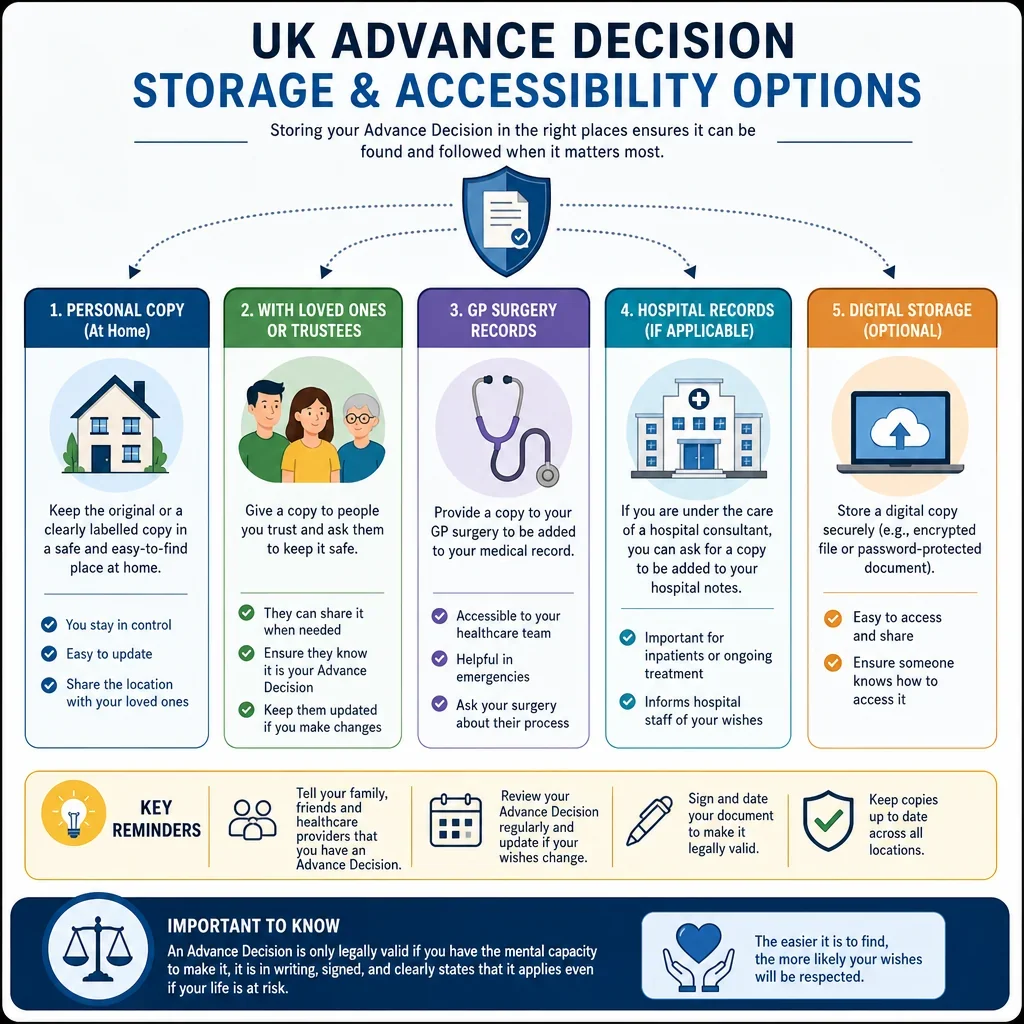
Where Should An Advance Decision Be Checked In UK Healthcare?
An Advance Decision is most likely to matter at points where treatment decisions are being made and the person may lack capacity, especially GP care, ambulance or emergency care, hospital admission, intensive care, palliative care, mental health services, and care homes.
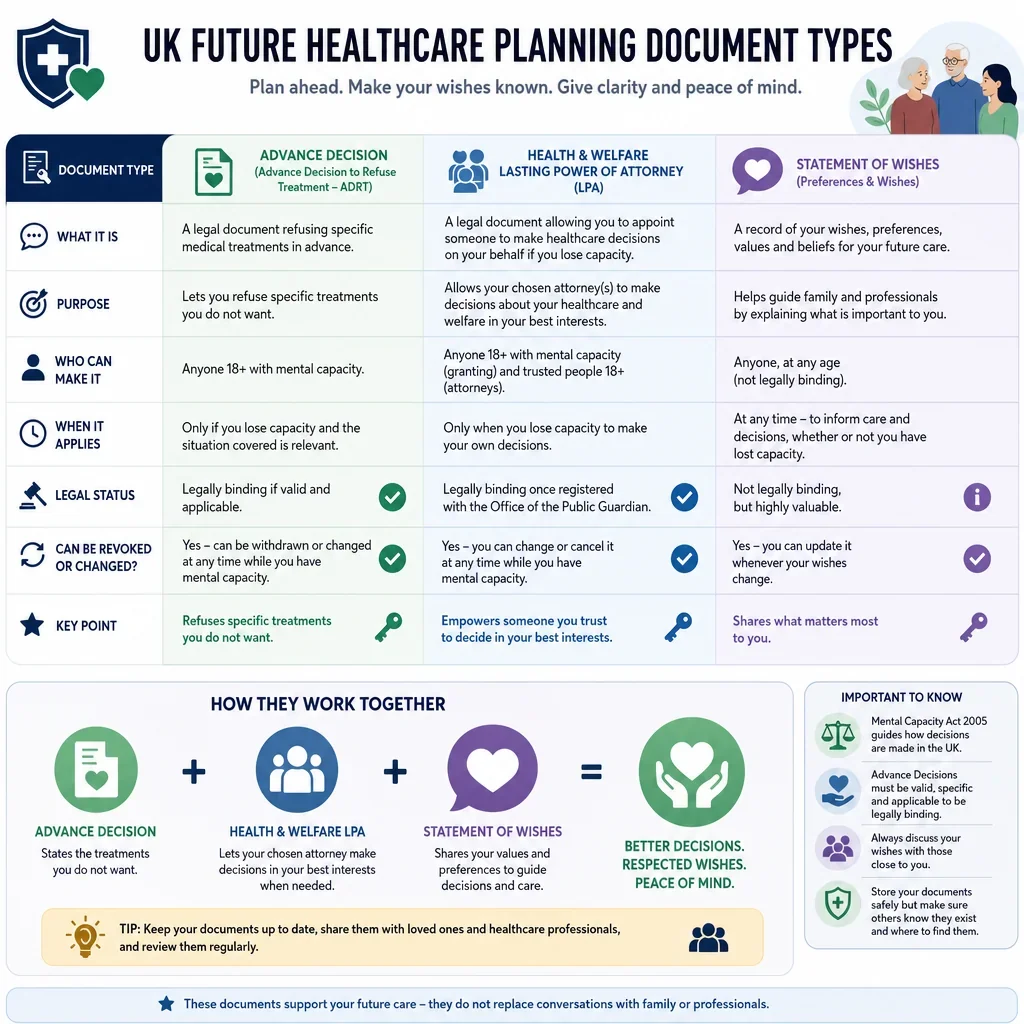
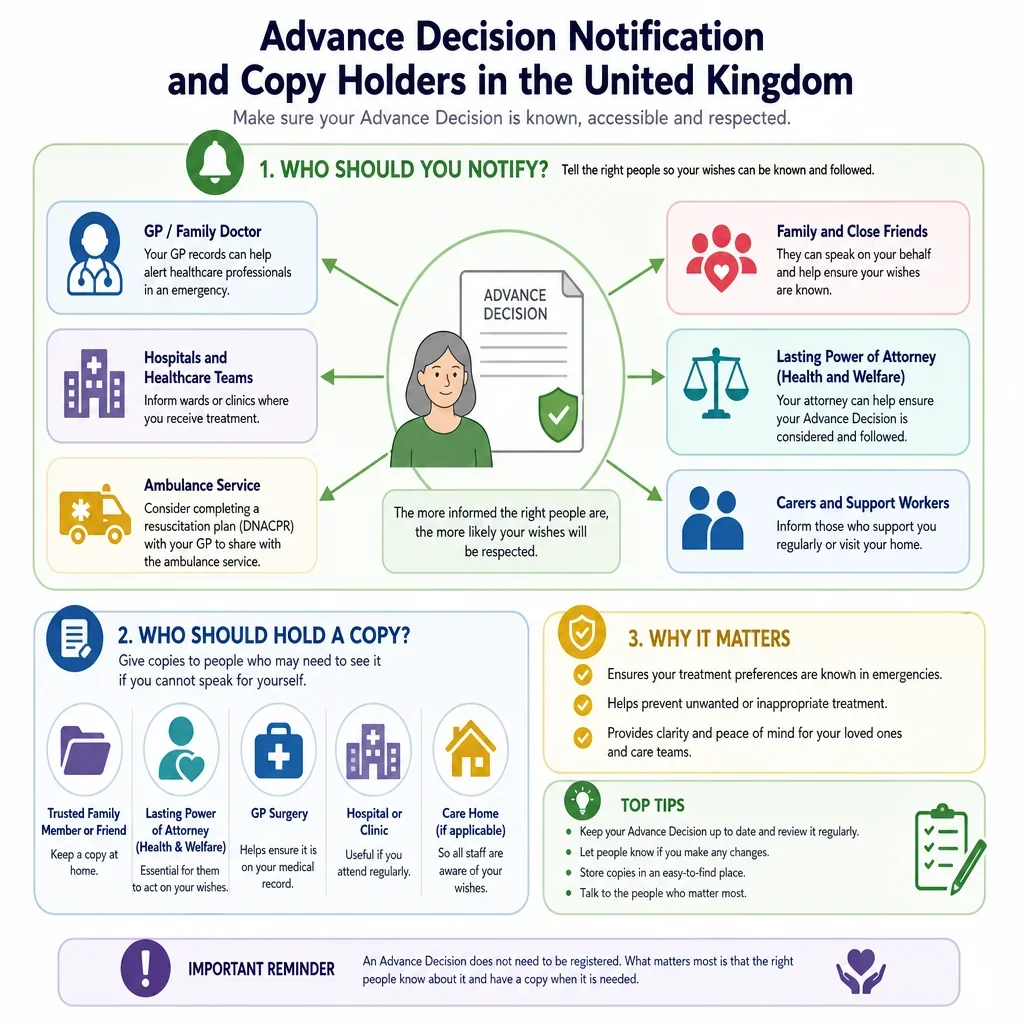
Who Needs To Know About An Advance Decision?
- GPs and hospital clinicians are often central because they record diagnoses, treatment plans and capacity assessments.
- Ambulance and emergency teams may need rapid access to reliable records before giving life-sustaining treatment.
- Care homes, community nurses and palliative care teams often help make sure the document is visible in day-to-day care planning.
- Records and administrative staff may not make treatment decisions, but accurate scanning, coding and flagging can affect whether clinicians see the document in time.
What Records Are Most Relevant To An Advance Decision?
Relevant UK records commonly include GP records, hospital electronic patient records, ambulance records, care plans, ReSPECT forms, DNACPR forms, mental health care plans, and discharge summaries. These records do not replace the legal document, but they can alert clinicians that an Advance Decision exists.
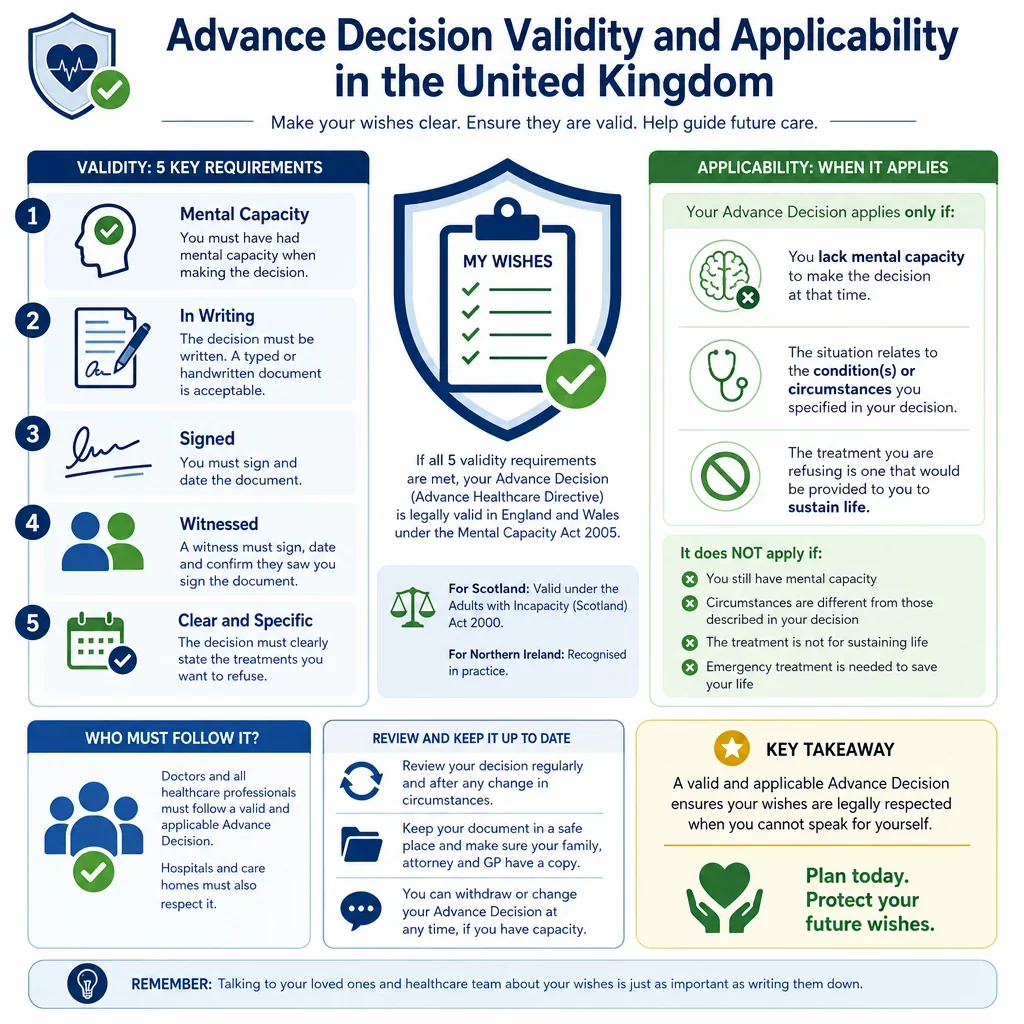
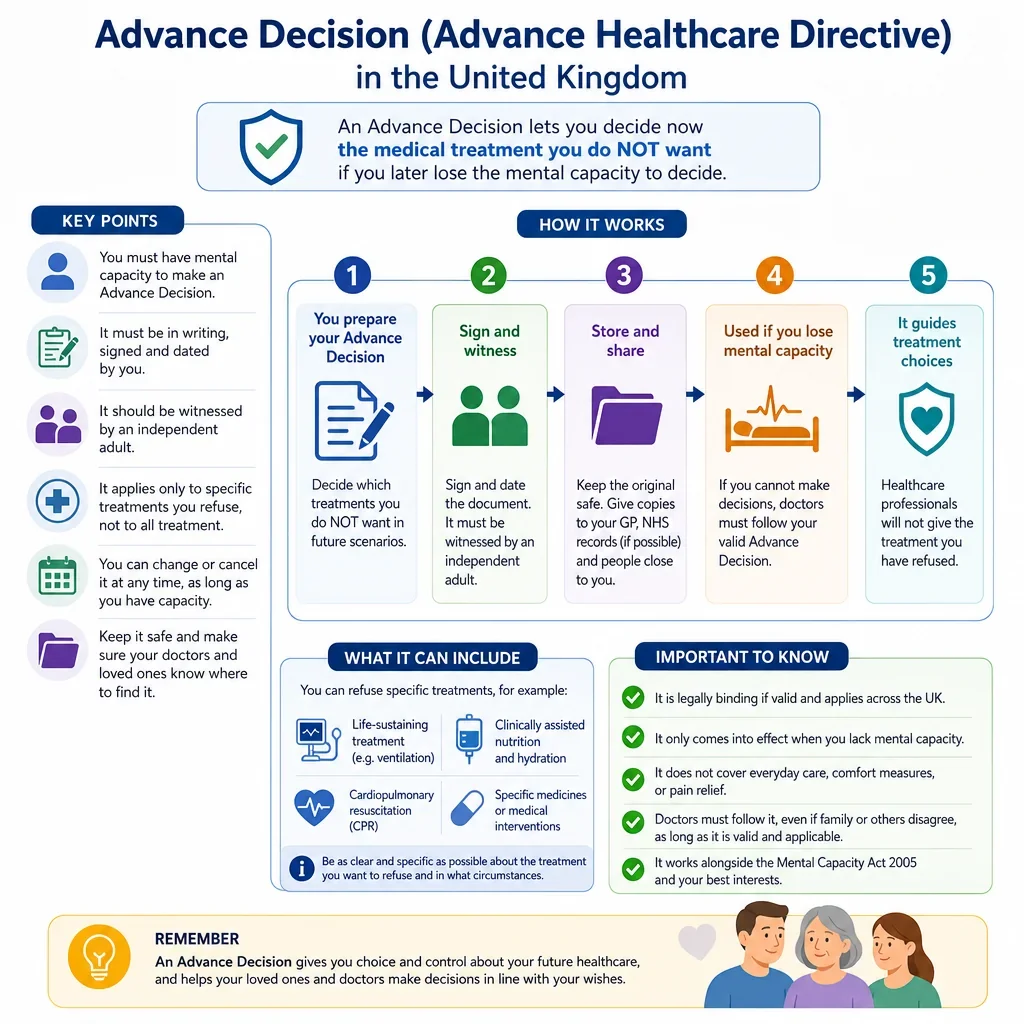
What Is The Key Legal Point For Clinicians?
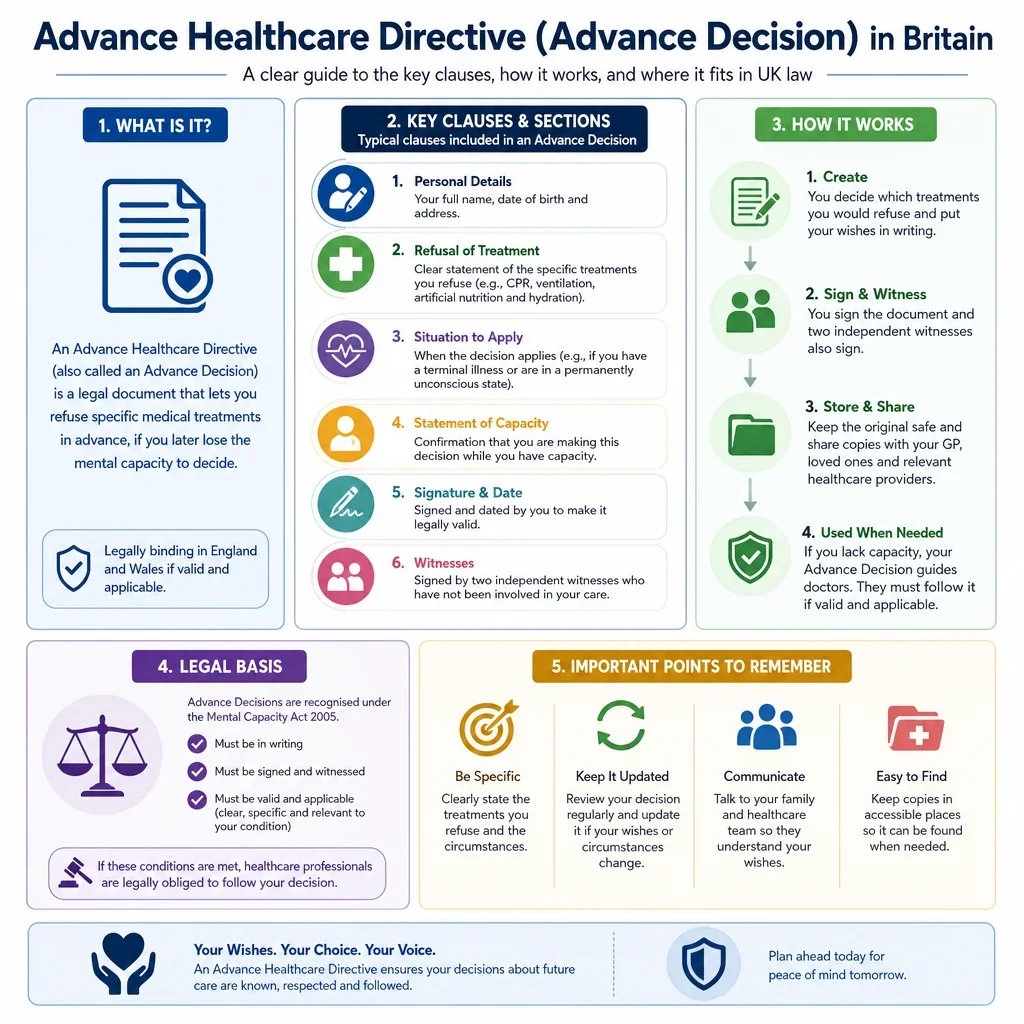
Under the Mental Capacity Act 2005, healthcare professionals must consider whether an Advance Decision is valid and applicable to the treatment in question at the relevant time. If it refuses life-sustaining treatment, it must meet additional statutory requirements, including being in writing, signed and witnessed, and stating that it applies even if life is at risk.
FAQs
You Might Also Be Interested In