Advance Healthcare Directive Clauses And Sections In Britain
Clause name | Purpose | Relevant to life sustaining treatment refusal | Drafting note |
|---|---|---|---|
Personal details | |||
Full Name And Identity Details | Identifies the person making the Advance Decision. | true | Include full name, date of birth, NHS number if known, and current address. |
Current Address And Contact Details | Helps clinicians match the document to the correct patient. | true | Add residential address, telephone number, email, and any previous names. |
Date Of Birth | Provides a key identifier for healthcare records. | true | Use day, month, and year to reduce risk of misidentification. |
NHS Number | Links the Advance Decision to NHS clinical records. | false | Include the NHS number if known do not delay signing solely to find it. |
Statement of understanding | |||
England And Wales Jurisdiction Statement | States the document is intended as an Advance Decision under the Mental Capacity Act 2005. | true | Use where the maker is in England or Wales or wants the document governed by that framework. |
Capacity At Time Of Making | Records that the maker has capacity when making the refusal. | true | State that the maker understands the nature and consequences of the decision. |
Understanding Of Consequences | Shows the maker understands the effect of refusing treatment. | true | Mention discussion with a clinician if one occurred and note likely outcomes. |
Free And Voluntary Decision | Records that the decision is made without pressure or coercion. | true | State that the maker has not been pressured by family, carers, or professionals. |
Treatment refusal | |||
Circumstances In Which Refusal Applies | Defines when the specified refusal is to operate. | true | Describe clinical situations clearly, such as permanent unconsciousness or advanced dementia. |
Specific Treatment Refused | Identifies the treatment the maker refuses in advance. | true | Name each treatment rather than using only broad wording where possible. |
Treatment refusal, Life-sustaining treatment wording | |||
Refusal Of Cardiopulmonary Resuscitation | Refuses attempted CPR in specified circumstances. | true | State whether CPR is refused only in defined conditions or in all future circumstances. |
Refusal Of Artificial Ventilation | Refuses mechanical ventilation or breathing support in specified circumstances. | true | Specify invasive ventilation, non-invasive ventilation, or both, if intended. |
Refusal Of Artificial Nutrition And Hydration | Refuses clinically assisted feeding or fluids in specified circumstances. | true | Use precise wording for tube feeding, intravenous fluids, or clinically assisted nutrition and hydration. |
Refusal Of Dialysis | Refuses kidney dialysis in specified circumstances. | true | State whether refusal covers starting dialysis, continuing dialysis, or both. |
Treatment refusal | |||
Refusal Of Antibiotics For Life-Threatening Infection | Refuses antibiotics where infection occurs in specified end-of-life conditions. | true | Clarify whether comfort-focused antibiotics remain acceptable. |
Refusal Of Blood Transfusion | Refuses transfusion of blood or blood products. | true | List any acceptable blood fractions or alternatives if relevant. |
Refusal Of Surgery Or Invasive Procedures | Refuses specified operations or invasive interventions. | false | Identify procedures and circumstances avoid refusing routine comfort measures unintentionally. |
Refusal Of Chemotherapy Or Cancer Treatment | Refuses specified cancer treatments in defined circumstances. | false | State whether the refusal covers curative, palliative, or experimental treatment. |
Refusal Of Intensive Care Admission | Refuses ICU-level treatment in stated circumstances. | true | Specify which ICU treatments are refused rather than refusing location alone. |
Palliative Care Not Refused | Confirms comfort care, pain relief, and symptom control are still wanted. | false | State that refusal of treatment does not refuse pain relief, nursing care, or hygiene. |
Basic Care Not Refused | Clarifies that ordinary care and comfort measures remain accepted. | false | Mention warmth, hygiene, mouth care, food and drink by mouth if safe, and pain relief. |
Emergency Treatment Pending Assessment | Allows urgent steps while validity and applicability are checked. | false | Acknowledge that clinicians may give emergency treatment while locating or verifying the document. |
Pregnancy Circumstances | States whether refusals apply if the maker is pregnant. | true | Include clear instructions if pregnancy would change the maker's decision. |
Statement of understanding | |||
Refusal Takes Effect When Capacity Is Lost | Confirms the refusal is intended to operate only if capacity is later absent. | true | State that the maker can decide for themselves while they have capacity. |
Life-sustaining treatment wording | |||
Applies Even If Life Is At Risk | Includes the required statement for refusing life-sustaining treatment. | true | Use clear words that the refusal applies even if life is at risk. |
Life-sustaining treatment wording, Witnessing and signature | |||
Written Form For Life-Sustaining Refusal | Records that the life-sustaining treatment refusal is in writing. | true | Ensure the refusal is contained in the signed written document, not only discussed orally. |
Witnessing and signature | |||
Maker Signature | Shows the maker has signed the Advance Decision. | true | Include signature, printed name, date, and place of signing. |
Signature By Another Person At Direction | Allows signing by another person in the maker's presence and at their direction. | true | Record why another person signed and that the maker directed the signature. |
Witness Signature | Evidences witnessing of the maker's signature or directed signature. | true | Add witness name, address, signature, date, and statement of witnessing. |
Independent Witness Details | Supports reliability of the signature and reduces later disputes. | true | Prefer an adult independent witness who is not pressuring or benefiting from the decision. |
Date Of Signing | Shows when the Advance Decision was made or confirmed. | true | Use a single clear date and avoid undated amendments. |
Statement of understanding | |||
Clinical Discussion Record | Records medical advice considered when making the document. | false | Name the GP or consultant, date of discussion, and key points understood. |
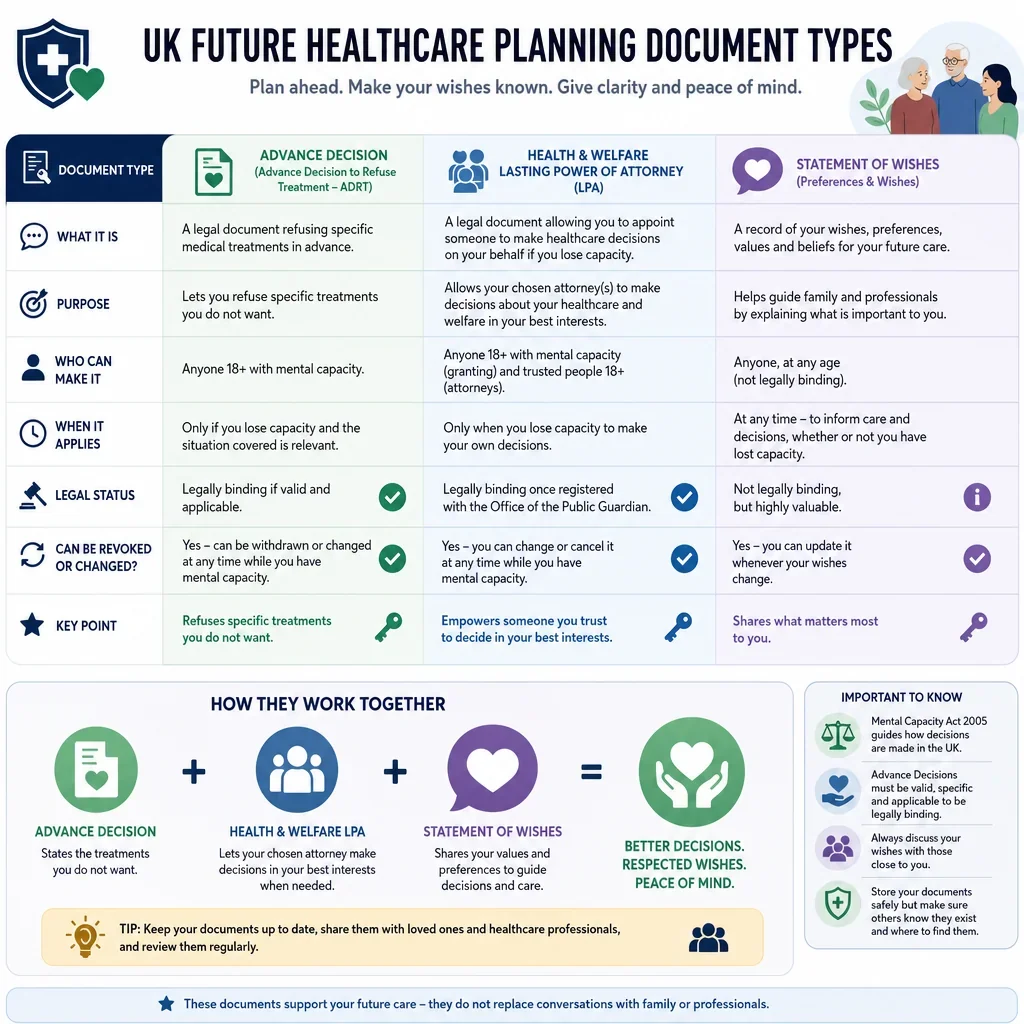
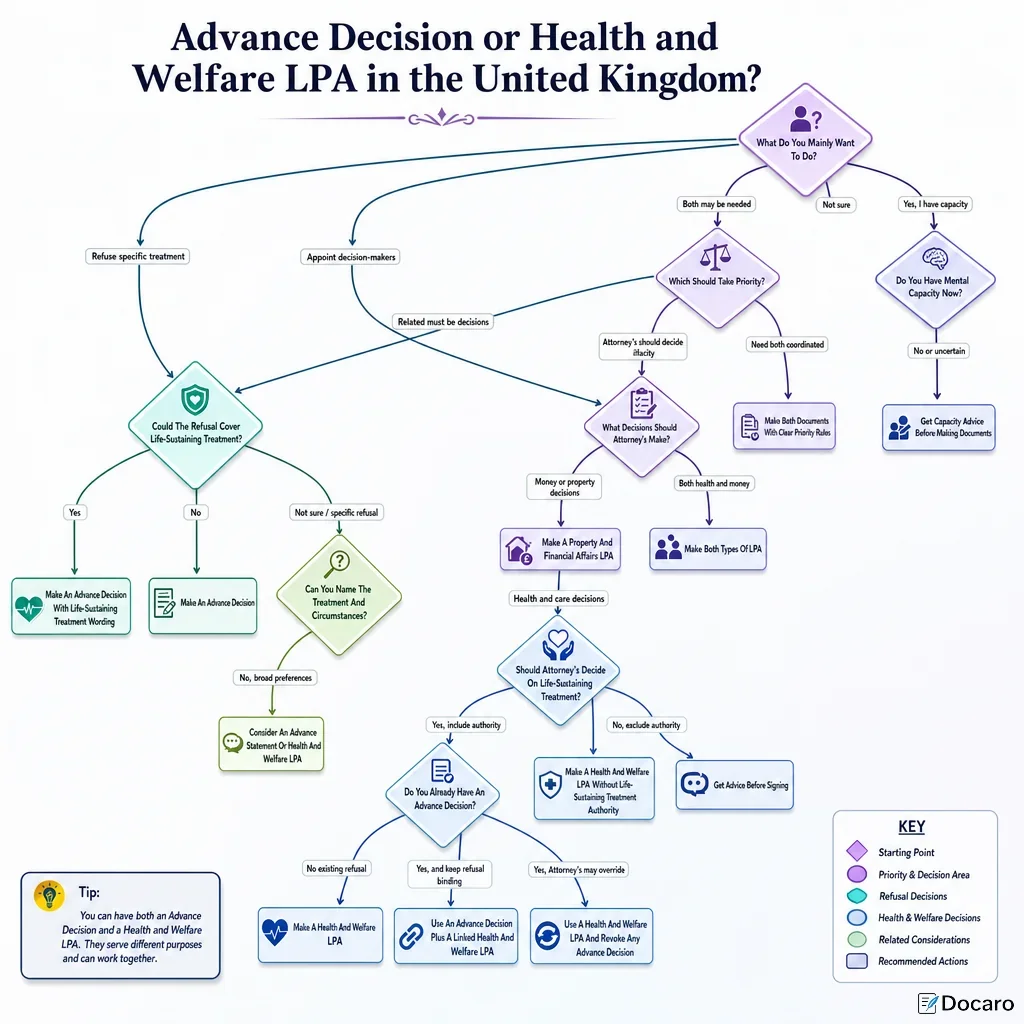
Health And Welfare LPA Compatibility | Clarifies the relationship with any health and welfare attorney authority. | true | State whether any LPA exists and whether it was made before or after this document. |
No Later Inconsistent Decision | Helps show the Advance Decision has not been withdrawn or overridden. | true | Confirm there is no later statement, conduct, or LPA authority inconsistent with the refusal. |
Review and updates | |||
Right To Withdraw While Capacitous | States the maker may withdraw the Advance Decision while they have capacity. | false | Explain that withdrawal can be made later and should be communicated clearly. |
Regular Review Schedule | Shows the document remains current and considered. | false | Include review intervals, such as annually or after major health changes. |
Review and updates, Witnessing and signature | |||
Review Confirmation Signature | Records that the maker has reviewed and confirmed the document. | false | Add review date, maker signature, and witness signature if practical. |
Review and updates | |||
Amendments And Replacement Versions | Prevents confusion between old and new versions. | false | Avoid handwritten changes sign a replacement document and destroy superseded copies. |
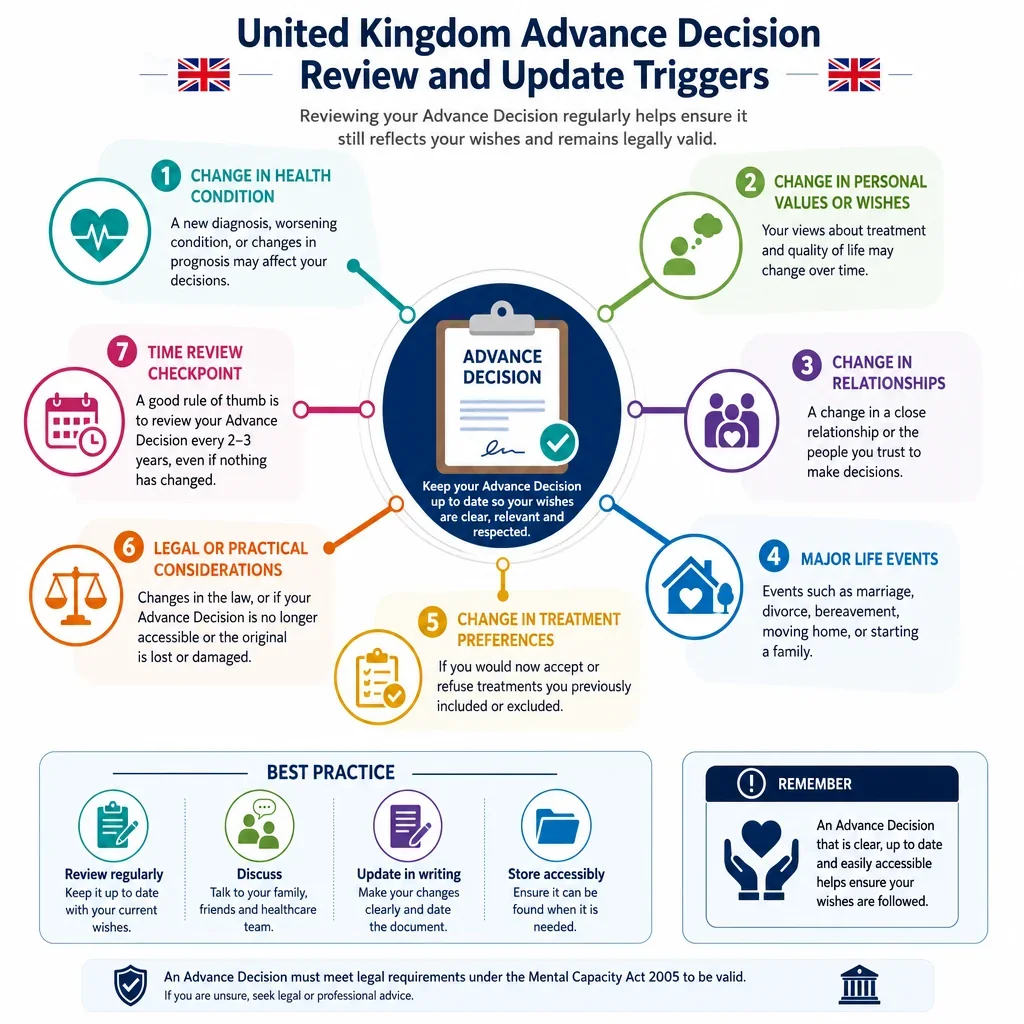
Review After Health Or Life Changes | Prompts review when circumstances may affect the maker's wishes. | false | List diagnosis, treatment change, hospitalisation, care move, relationship change, or new LPA. |
Communication and copies | |||
Copy To GP | Helps ensure the Advance Decision is noted in primary care records. | false | Name the GP practice and request that a copy is added to the medical record. |
Copy To Hospital Or Specialist Team | Alerts treating specialists to treatment refusals relevant to future care. | false | List consultant, clinic, hospital, or community team receiving a copy. |
Copy To Care Home Or Carers | Ensures day-to-day carers know the document exists. | false | Identify the care provider and where the copy should be stored. |
Notification To Health And Welfare Attorneys | Informs attorneys of treatment refusals and document location. | false | List attorney names, contact details, and whether they hold a registered LPA. |
Family And Emergency Contact Notification | Reduces delay and dispute by identifying people who know about the document. | false | Include names, relationships, phone numbers, and whether each person has a copy. |
Location Of Original Document | Helps clinicians or relatives locate the signed original quickly. | false | State the storage place and who can access it in an emergency. |
List Of Copy Holders | Shows who has received the Advance Decision. | false | Record names, roles, addresses or emails, and date sent. |
Electronic Record And Digital Copy | Encourages accessible digital storage alongside paper copies. | false | Note if a scanned copy is held by GP, hospital, attorney, or secure cloud account. |
Wallet Card Or Emergency Notice | Alerts emergency staff that an Advance Decision exists. | false | Include maker name, emergency contact, GP, and location of the signed document. |
Ambulance And Emergency Services Information | Helps emergency responders identify refusals relevant to urgent treatment. | false | Ask the GP or care team about local electronic palliative care or urgent care records. |
Communication and copies, Treatment refusal | |||
Relationship With DNACPR Form | Clarifies whether a separate DNACPR record exists or is requested. | true | State that the Advance Decision is distinct from, but may support, CPR planning. |
Statement of understanding | |||
Values And Reasons Statement | Explains the values behind the treatment refusals. | false | Keep separate from binding refusals and avoid unclear conditions. |
Advance Statement Is Non-Binding | Distinguishes preferences from legally binding treatment refusals. | false | Label wishes about place of care, visitors, or beliefs as preferences, not refusals. |
No Request For Assisted Dying | Clarifies the document refuses treatment and does not request unlawful assisted dying. | false | State that the maker seeks lawful refusal of treatment, not active steps to cause death. |
Mental Health Act Treatment Caveat | Notes limits where treatment is regulated by mental health legislation. | false | Include if the maker has relevant mental health history or wants to avoid overstatement. |
No Demand For Specific Treatment | Confirms an Advance Decision refuses treatment and cannot require treatment. | false | Put treatment preferences in an advance statement or care plan instead. |
Review and updates | |||
Change In Circumstances Warning | Recognises that changed circumstances may affect applicability. | true | Review wording if treatments, diagnosis, prognosis, or personal wishes change. |
Statement of understanding | |||
If Validity Or Applicability Is Unclear | Acknowledges clinicians must consider validity and applicability before relying on refusal. | false | Name contacts who can confirm wishes, but do not give them power to alter the refusal. |
Treatment refusal | |||
Medical Conditions Covered | Links refusals to specified current or future medical conditions. | true | Use plain descriptions and clinical terms where known, such as MND, dementia, stroke, or cancer. |
Treatment refusal, Life-sustaining treatment wording | |||
Permanent Unconsciousness Or Coma Scenario | Applies refusals if recovery of consciousness is not expected. | true | Define who should assess prognosis, such as the responsible consultant and a second doctor. |
Advanced Dementia Scenario | Applies refusals if dementia reaches a defined severe stage. | true | Describe functional triggers, such as inability to recognise family or swallow safely. |
Terminal Illness Scenario | Applies refusals where illness is incurable and death is expected. | true | Define prognosis threshold if desired, such as days, weeks, or months. |
Severe Stroke Or Brain Injury Scenario | Applies refusals after catastrophic neurological injury in defined circumstances. | true | Describe outcomes that would trigger refusal, such as permanent inability to communicate. |
Treatment refusal | |||
Severe Irreversible Suffering Scenario | Applies refusals where suffering is severe and cannot be acceptably relieved. | true | Define suffering carefully and include clinical assessment requirements where possible. |
Statement of understanding | |||
Religious Or Ethical Basis | Records beliefs relevant to the refusal, such as blood product decisions. | false | Keep belief statements concise and connect them to specific treatment refusals. |
Statement of understanding, Witnessing and signature | |||
Interpreter Or Communication Support Used | Shows communication support was provided when making the decision. | false | Record interpreter name, method used, and confirmation that the maker understood. |
Statement of understanding | |||
Capacity Assessment Attachment | Provides extra evidence of capacity where challenge is possible. | false | Consider a clinician note if the maker has cognitive impairment or complex refusals. |
Binding Refusal Not Best Interests Preference | States that a valid and applicable refusal must be followed, not balanced as a preference. | true | Use for clarity where the maker wants binding refusal rather than general guidance. |
Treatment refusal | |||
Treatments Not Covered | Clarifies which treatments are not refused by the document. | false | List treatments the maker still accepts to reduce unintended broad interpretation. |
Communication and copies | |||
Organ Donation Compatibility | Notes whether refusals should be read consistently with organ donation wishes. | false | State whether short-term procedures for organ donation are accepted or refused. |
Person To Contact About Wishes | Identifies someone who can explain the maker's wishes and document history. | false | Make clear the contact explains wishes only and does not override a valid refusal. |
Statement of understanding | |||
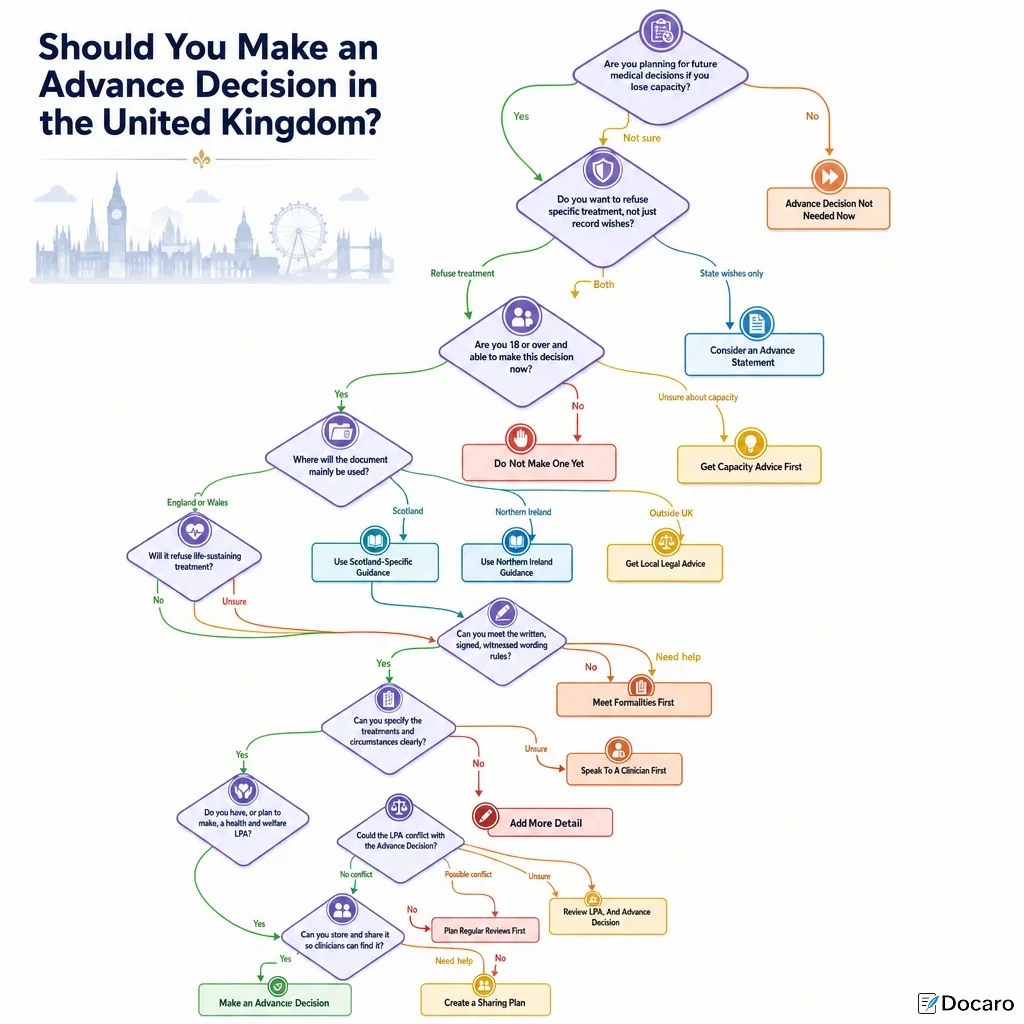
Scotland And Northern Ireland Caution | Warns that legal rules differ outside England and Wales. | false | Use jurisdiction-specific advice if the maker lives, receives care, or travels elsewhere in the UK. |
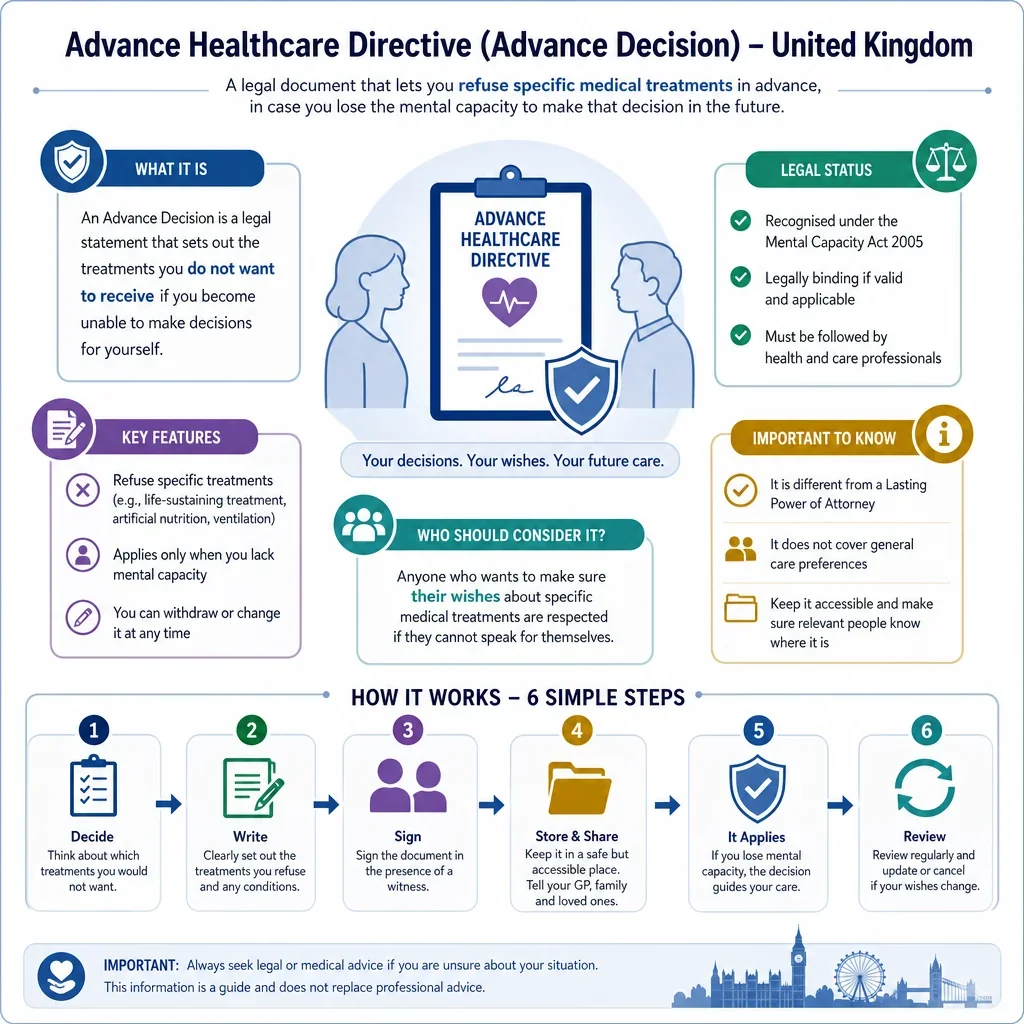
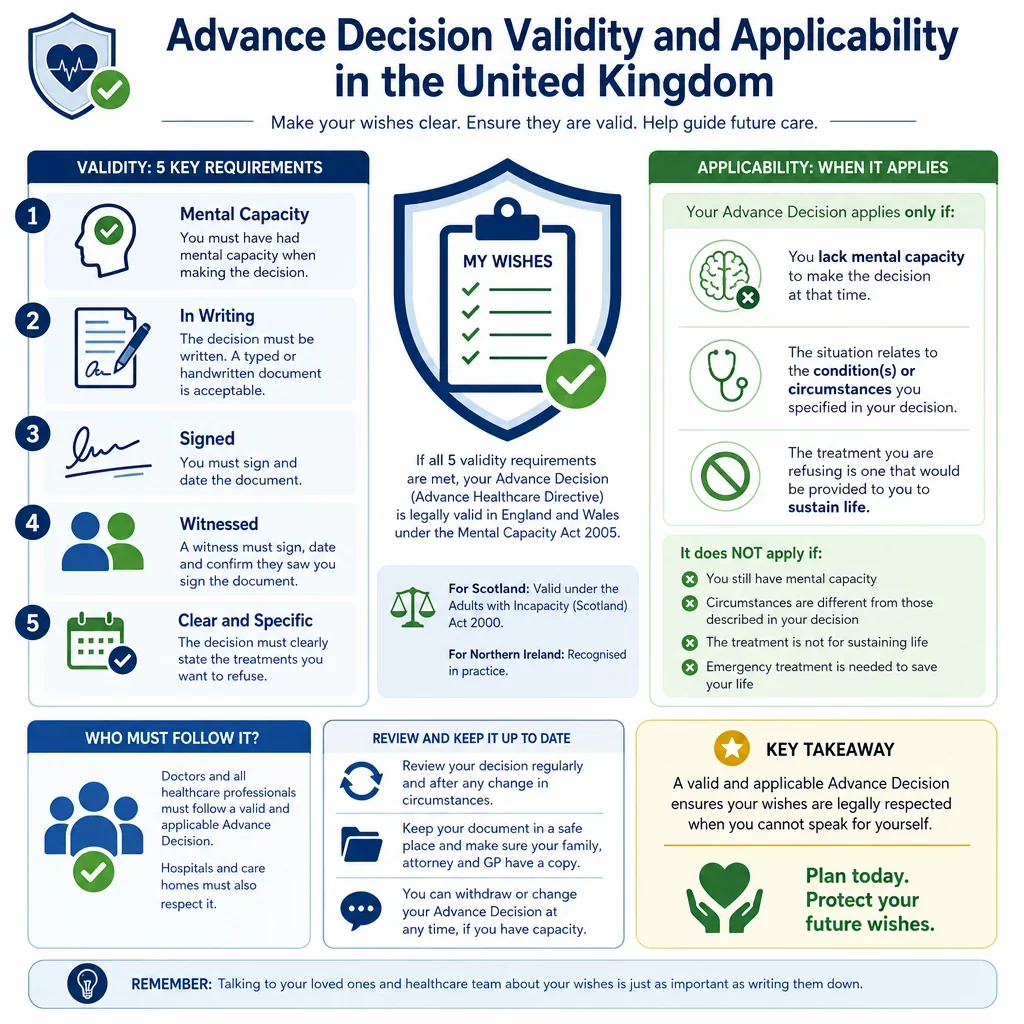
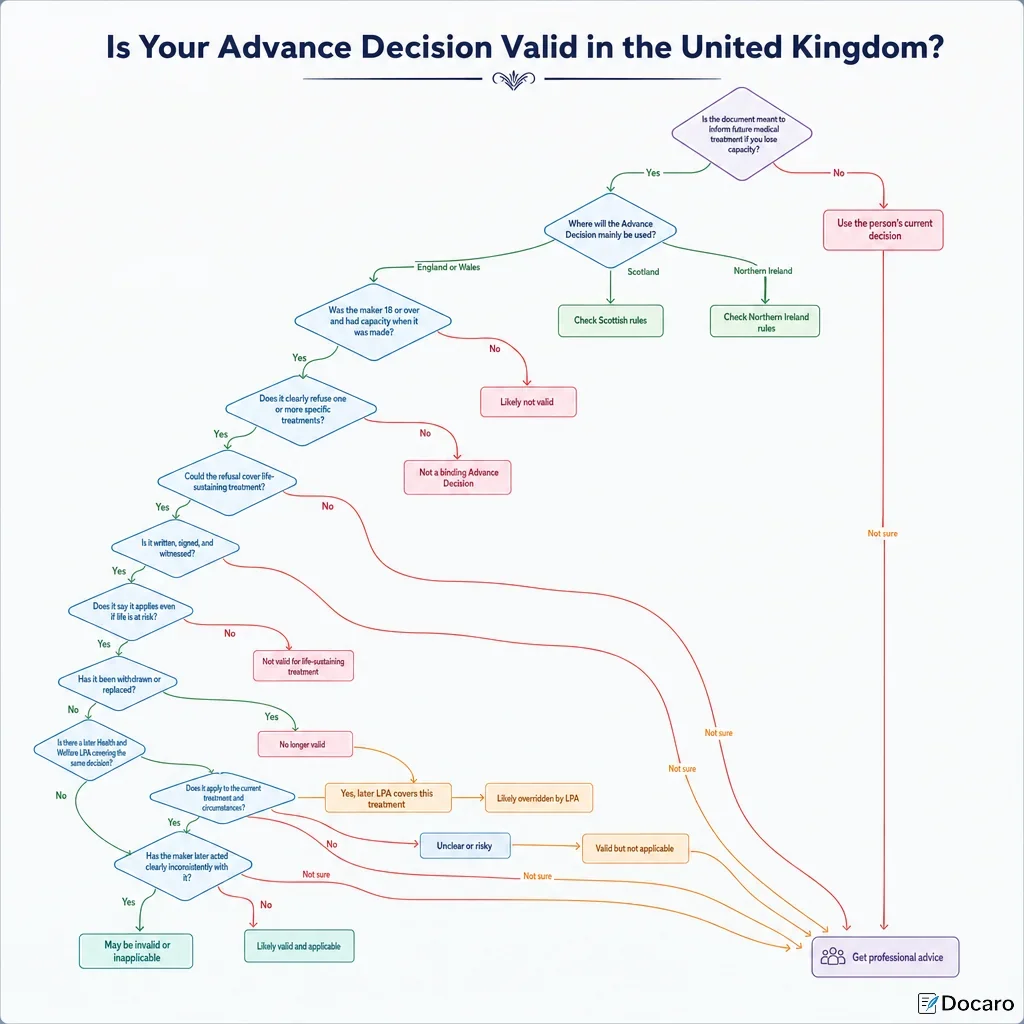
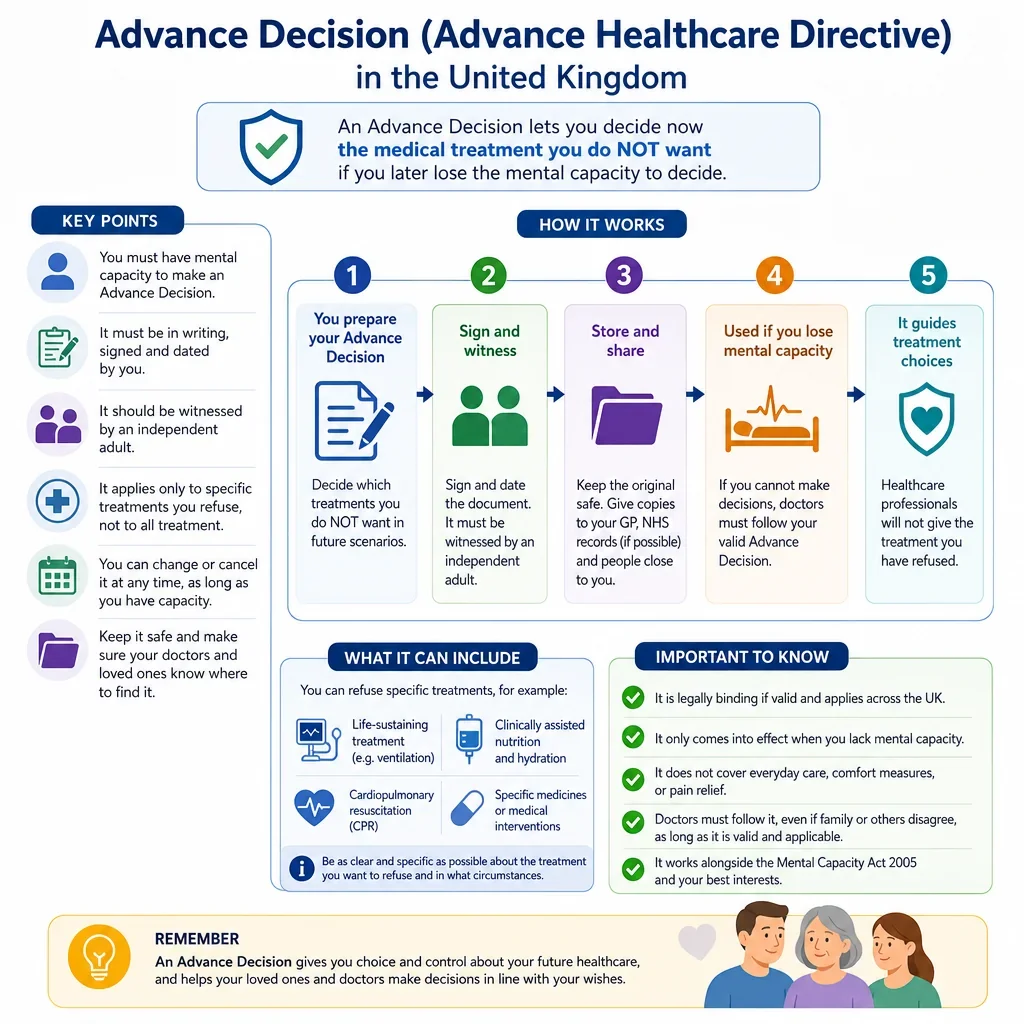
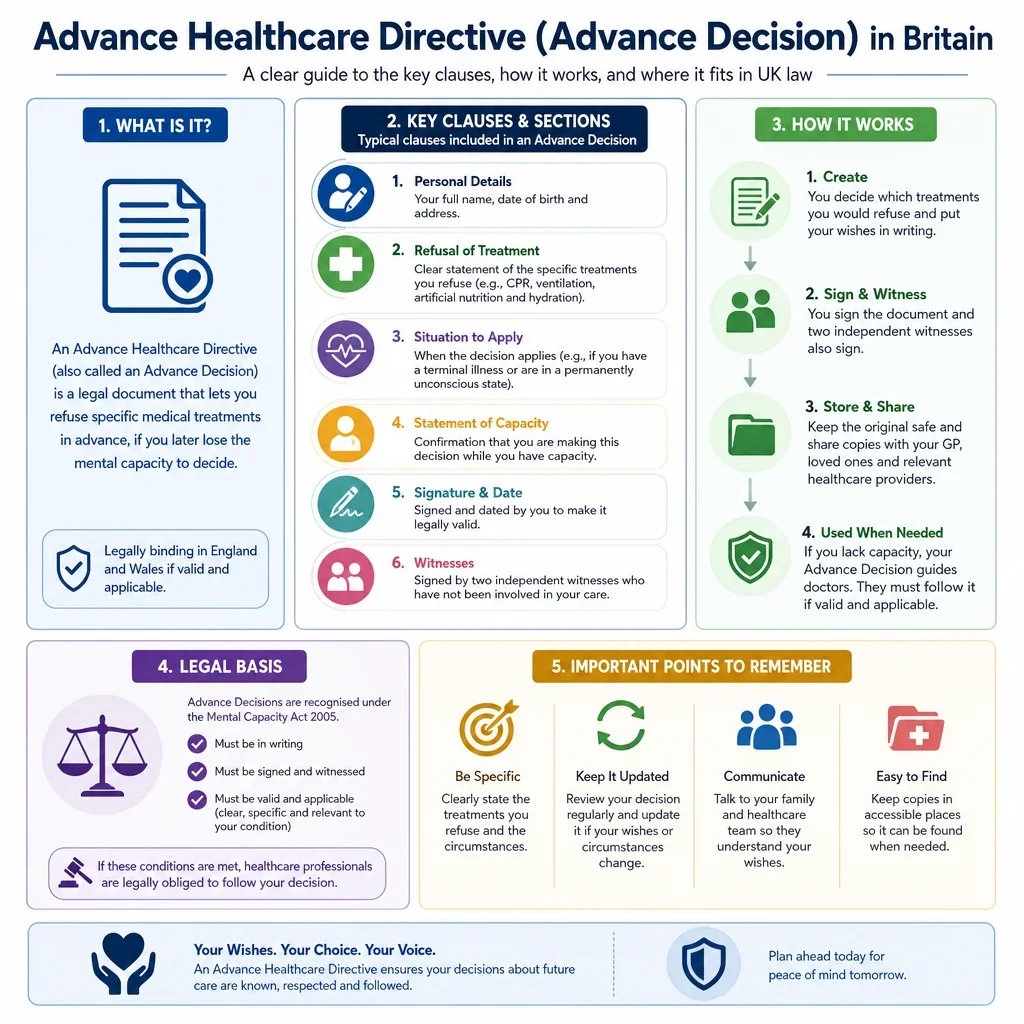
What Clauses Make An Advance Decision Valid In England And Wales?
An Advance Decision to refuse treatment should clearly identify the maker, specify the treatment refused, and state the circumstances in which the refusal applies. If it refuses life-sustaining treatment, it must be in writing, signed by the maker or by someone at the maker's direction, witnessed, and include an express statement that the refusal is to apply even if life is at risk.
Which Clauses Are Most Important For Refusing Life-Sustaining Treatment?
- Life-sustaining treatment wording is critical: the document should say the refusal applies even if life is at risk.
- Specific treatment refusal clauses help avoid uncertainty by naming treatments such as CPR, ventilation, artificial nutrition and hydration, dialysis, antibiotics, or blood transfusion where relevant.
- Witnessing and signature clauses are especially important because special formalities apply to life-sustaining treatment refusals.
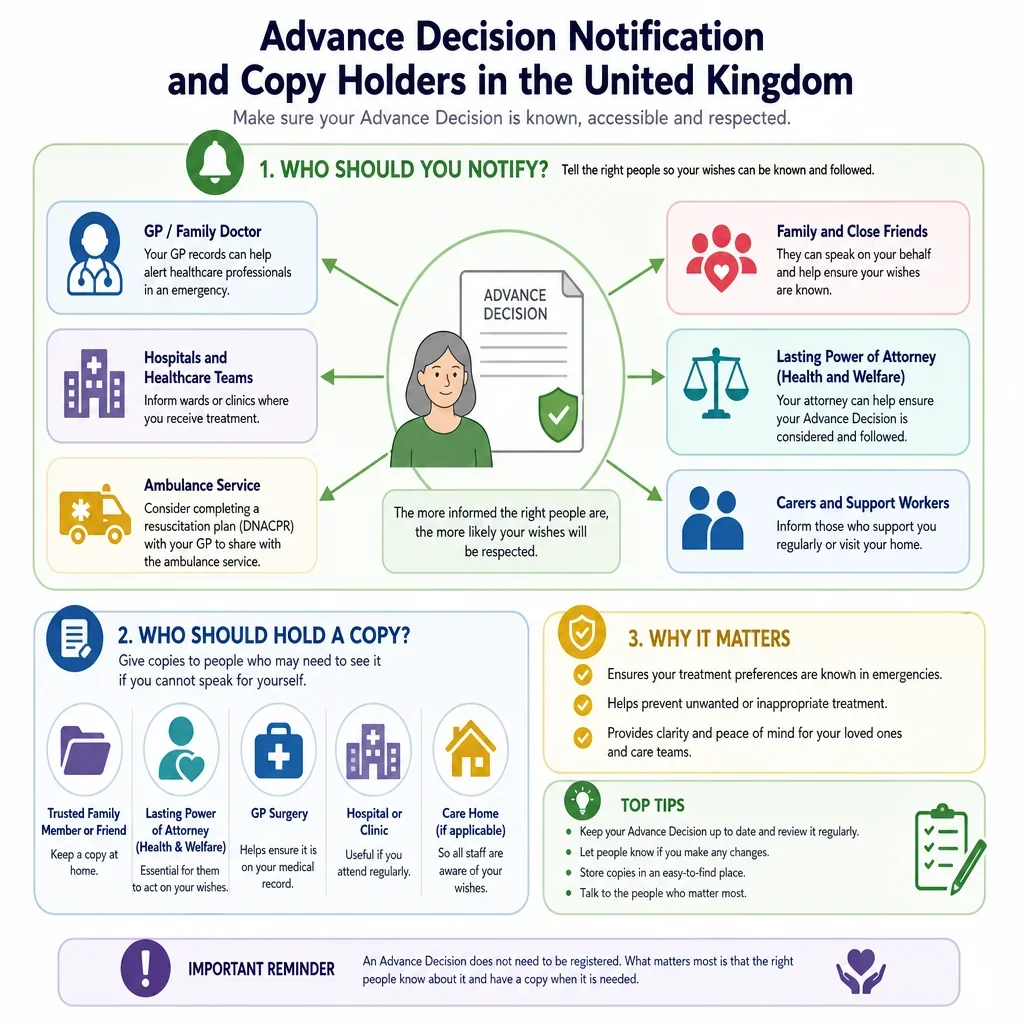
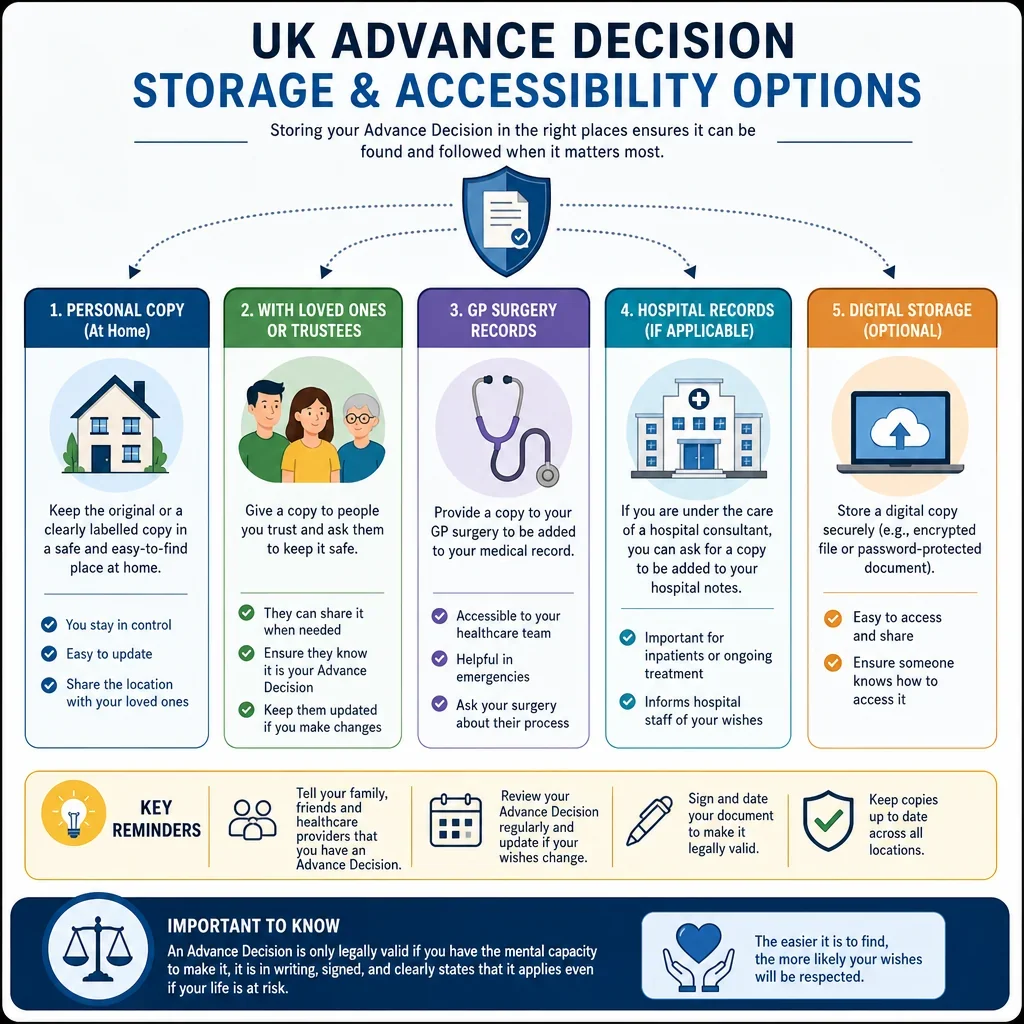
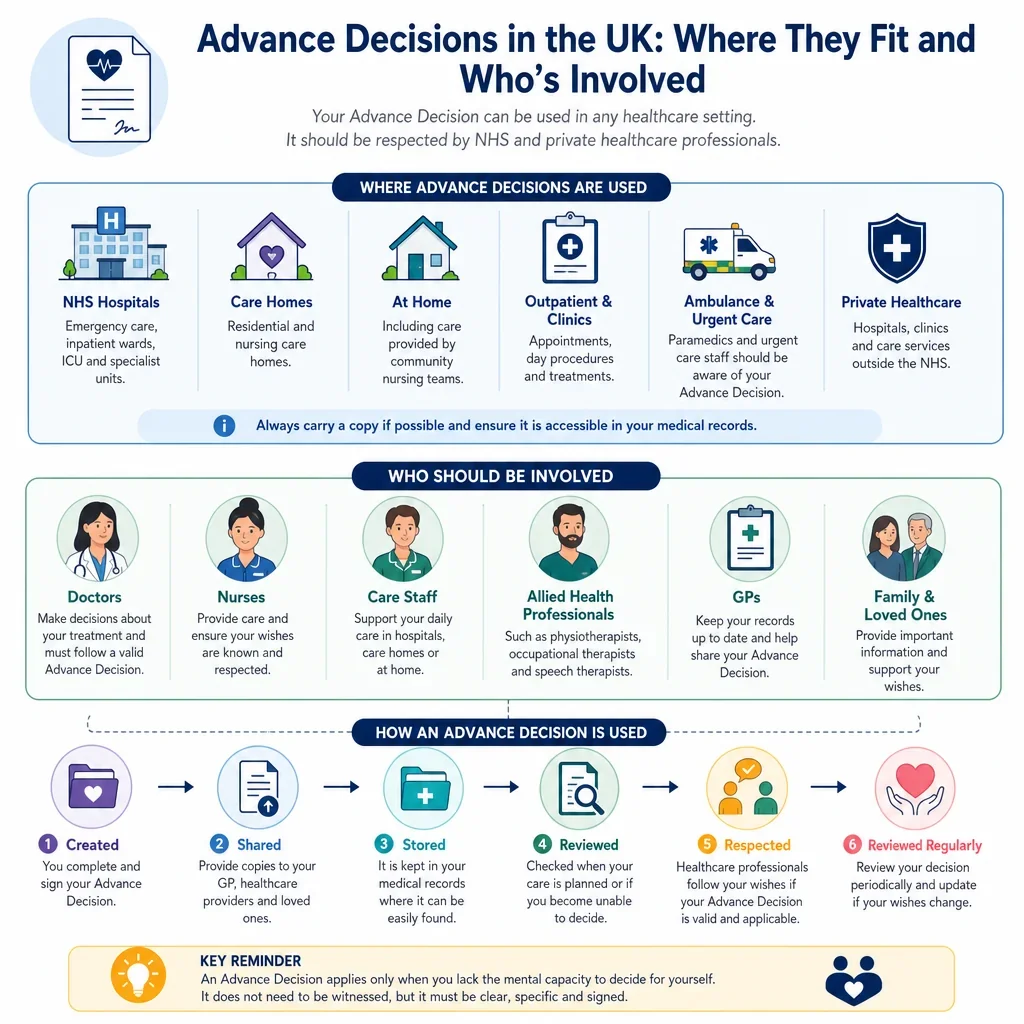
How Should Copies And Communication Be Handled?
The document is more useful if it includes clauses for sharing copies with the GP, hospital team, care home, family members, attorneys under a health and welfare LPA, and emergency contacts. A clause stating where the original is kept can help clinicians find and rely on it quickly.
Why Should An Advance Decision Be Reviewed?
Regular review clauses help show that the decision still reflects the maker's wishes. A review is particularly useful after a new diagnosis, change in treatment options, hospital admission, care home move, marriage or civil partnership change, or creation of a health and welfare lasting power of attorney.
What Should Users Know About UK Differences?
The statutory Advance Decision rules in the Mental Capacity Act 2005 apply in England and Wales. Scotland and Northern Ireland use different legal frameworks and terminology, so a UK-facing document should make clear which jurisdiction it is intended for.
FAQs
You Might Also Be Interested In