Advance Decision Validity And Applicability Checklist In The United Kingdom
Requirement | Explanation | Especially relevant to life sustaining treatment | Suggested action |
|---|---|---|---|
Legal validity | |||
Maker must be 18 or over | An Advance Decision can only be made by an adult. | false | Record the maker's full name, date of birth and address. |
Capacity | |||
Maker must have capacity when making it | A person cannot make a valid Advance Decision unless they can understand, retain, use or weigh the relevant information and communicate the decision. | true | Consider a capacity note from a GP or clinician for serious refusals. |
Legal validity | |||
Specific treatment must be refused | The document must say which treatment is refused, not just express a general wish. | true | Name treatments such as CPR, ventilation, dialysis, antibiotics or artificial nutrition and hydration. |
Applicability | |||
Circumstances must be clearly identified | A refusal only applies if the current circumstances match those described in the Advance Decision. | true | Describe diagnoses, stages of illness, symptoms or loss of abilities that trigger the refusal. |
Legal validity | |||
Life-sustaining refusal must be in writing | A refusal of life-sustaining treatment is not valid unless recorded in writing. | true | Use a written document rather than relying on spoken instructions. |
Life-sustaining refusal must be signed | The maker must sign, or direct another person to sign in their presence. | true | Sign and date the final version clearly. |
Witnessing | |||
Signature must be witnessed for life-sustaining refusal | The witness confirms the signature or directed signature was made properly. | true | Ask an independent adult witness to sign and add their name, address and date. |
Legal validity | |||
Must say it applies even if life is at risk | A life-sustaining treatment refusal needs an express statement that it applies even if life is at risk. | true | Include wording such as: I refuse this treatment even if my life is at risk. |
Applicability | |||
Maker must lack capacity when treatment decision arises | An Advance Decision is used only when the person cannot make or communicate the treatment decision at the time. | true | If you have capacity, tell clinicians your current decision directly. |
Current treatment must match the refused treatment | Clinicians must be able to see that the treatment now proposed is covered by the refusal. | true | Use both common and clinical names for key treatments where possible. |
Current circumstances must match the document | A valid refusal may still not apply if the situation is materially different from the one described. | true | Avoid vague triggers and define the medical situations you mean. |
Legal validity | |||
It must not have been withdrawn | An Advance Decision is invalid if the maker withdrew it while they had capacity. | true | If revoking it, destroy old copies and tell your GP, attorneys and family. |
No later conflicting health and welfare LPA | A later LPA may override an Advance Decision if it gives the attorney authority over the same treatment. | true | Check any health and welfare LPA is consistent with the Advance Decision. |
No later conduct clearly inconsistent with it | The document may be invalid if the maker later acted in a way clearly inconsistent with the refusal. | true | Review the document after major life, health or belief changes. |
Applicability | |||
No reasonable grounds that circumstances were unanticipated | A refusal may not apply if later developments make it reasonable to think the maker would have reconsidered. | true | Update it when new treatments, diagnoses or prognosis information arise. |
Legal validity | |||
It cannot demand treatment | An Advance Decision refuses specified treatment it does not require clinicians to provide requested treatment. | false | Put treatment preferences in a separate advance statement or care plan. |
It cannot request assisted dying | It can refuse treatment but cannot require anyone to take steps to end life. | true | Focus wording on refusals of specified medical treatment. |
Communication | |||
Oral refusals are limited | A spoken Advance Decision may be valid for non-life-sustaining treatment, but not for life-sustaining treatment. | true | Record all refusals in writing to avoid uncertainty. |
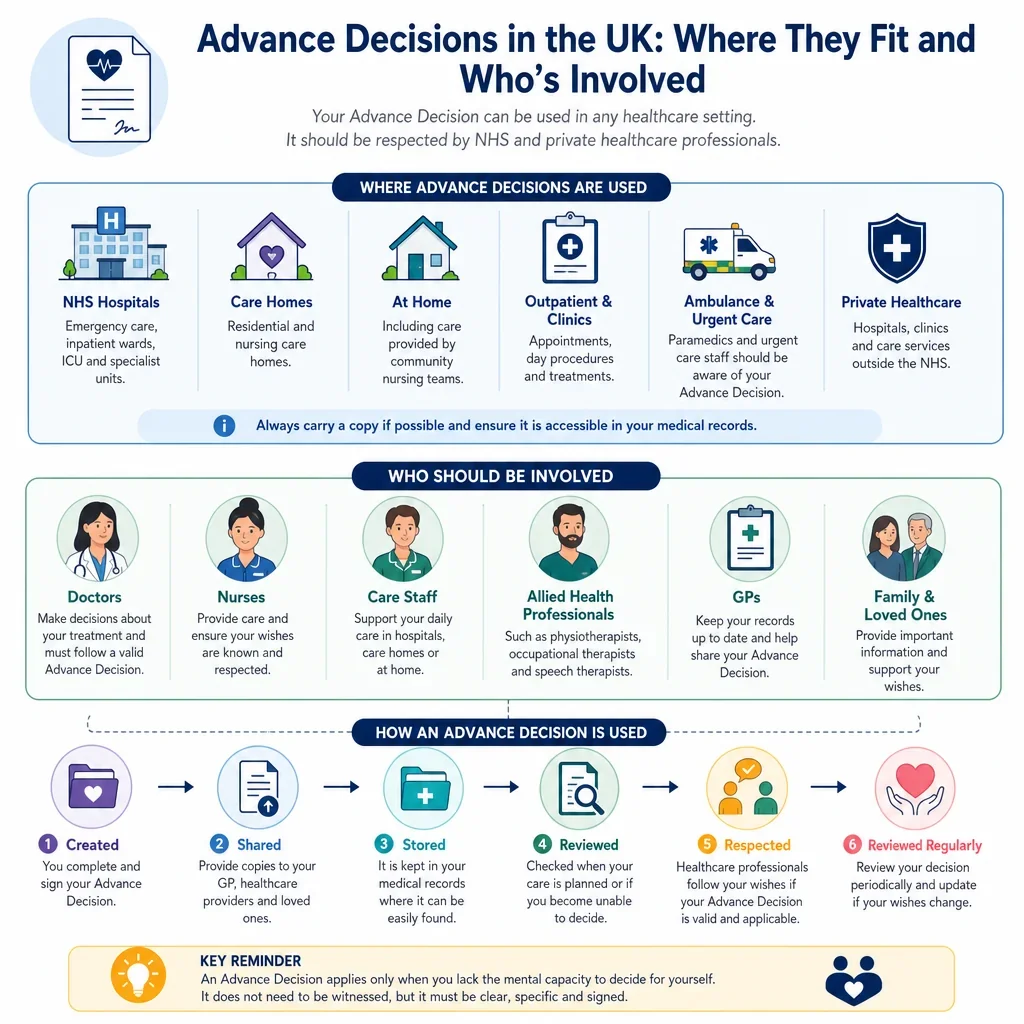
Clinicians must be able to find it | A valid document may not be applied in an emergency if healthcare staff do not know it exists. | true | Give copies to your GP, hospital team, care home and emergency contacts. |
Emergency contacts should be listed | Contacts can help clinicians locate the document and understand its background. | true | List trusted contacts, attorneys, GP details and where the original is stored. |
Family and carers should know about it | People close to the maker may be asked about wishes and whether the document is current. | true | Discuss the decision with key relatives, carers and any appointed attorney. |
Legal validity | |||
Date should be clearly recorded | The date helps show whether the document came before or after an LPA or later changes. | true | Date every signature, witness signature, review and replacement copy. |
Applicability | |||
Reasons and values should be included | Reasons help clinicians decide whether the refusal applies to the situation now faced. | true | Briefly explain the outcomes or burdens you are trying to avoid. |
Legal validity | |||
Wording must not be ambiguous | Ambiguous wording makes it harder to decide whether the refusal is valid and applicable. | true | Avoid phrases such as no heroic measures unless you define them precisely. |
Applicability | |||
CPR refusal should be clearly linked to the Advance Decision | CPR is life-sustaining treatment, so a refusal needs the life-risk statement and proper formalities. | true | Discuss CPR refusal with your clinician and ask how it should be recorded locally. |
Artificial nutrition and hydration should be named if refused | Clinically assisted nutrition and hydration may be treated as medical treatment and should be specified if refused. | true | State whether tube feeding, IV fluids or clinically assisted hydration are refused. |
Antibiotics or infection treatment should be specified if refused | Infections are common triggers for treatment decisions in advanced illness. | true | Say whether antibiotics are refused in all cases or only in defined end-stage situations. |
Ventilation refusal should distinguish invasive and non-invasive support | Breathing support can range from masks to intubation, so precise wording reduces disputes. | true | State whether you refuse intubation, mechanical ventilation, NIV, CPAP or all respiratory support. |
Dialysis refusal should define the condition covered | Dialysis may be temporary or long term, so circumstances matter. | true | Say whether refusal applies to acute kidney injury, chronic kidney failure or both. |
Blood product refusal should be precise | Different blood components may be acceptable or refused for different reasons. | true | List whether whole blood, red cells, plasma, platelets or derivatives are refused. |
Implanted device treatment should be addressed if relevant | Devices such as ICDs may affect end-of-life treatment decisions. | true | Discuss ICD deactivation or device settings with your cardiology team. |
Pain relief should not be accidentally refused | Refusing life-sustaining treatment does not normally mean refusing comfort care. | true | State that symptom relief, nursing care and comfort care are still wanted if that is your wish. |
Pregnancy-related wishes should be addressed if relevant | Pregnancy may create circumstances the maker might want treated differently. | true | Say whether the refusal changes during pregnancy or childbirth. |
Mental Health Act powers may affect treatment | The Mental Capacity Act does not override treatment powers under the Mental Health Act 1983. | false | Get specialist advice if the refusal concerns compulsory mental health treatment. |
If not valid and applicable, best interests decision applies | If the Advance Decision cannot be relied on, treatment decisions are made under best interests rules. | true | Make the document clear and share it so clinicians do not need to rely on fallback rules. |
Legal validity | |||
Valid and applicable refusal has the same effect as a current refusal | Healthcare professionals must respect a valid and applicable Advance Decision as if the person had made it now. | true | Use direct refusal wording rather than preferences or hopes. |
Applicability | |||
Emergency treatment may be given while checking validity | Clinicians may treat to prevent serious deterioration while deciding whether an Advance Decision exists and applies. | true | Carry an alert card and ensure records flag the document. |
Communication | |||
Only the current version should circulate | Multiple versions can create doubt about the maker's current wishes. | true | Mark replacements as current, withdraw old copies and keep a distribution list. |
Review | |||
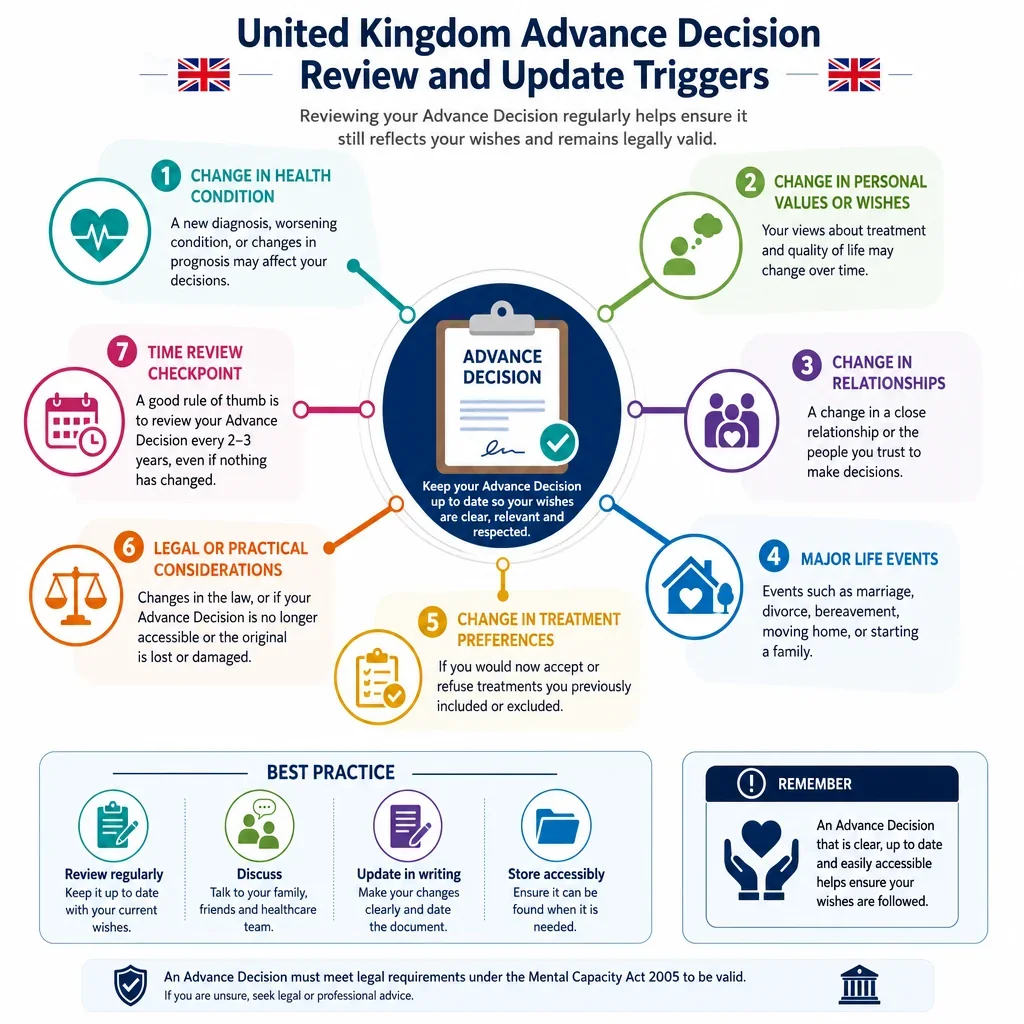
Regular review is strongly advisable | Review helps show the decision still reflects current wishes and circumstances. | true | Review at least every few years and after major medical or personal changes. |
Review after diagnosis or prognosis changes | New medical information may affect whether the original refusal still applies. | true | Ask a clinician to review the wording after a serious diagnosis or change in prognosis. |
Review when treatment options change | A new, less burdensome treatment could make old wording less certain. | true | Update the document if a new treatment would change your decision. |
Review after making or changing an LPA | A later health and welfare LPA can affect the legal status of the Advance Decision. | true | Ensure the LPA and Advance Decision say who decides about the same treatments. |
Review after major relationship changes | Relationship changes may affect contacts, attorneys and who knows your wishes. | false | Update contact details and send the new version to relevant people. |
Witnessing | |||
Witness should be independent where possible | Independence helps avoid later allegations of pressure or uncertainty. | true | Use an adult witness who is not a beneficiary, attorney or close family member if possible. |
Witness should be present when the maker signs | For life-sustaining treatment refusals, the witness must witness the signature or directed signature. | true | Sign in the witness's presence and have them sign immediately afterwards. |
Legal validity | |||
Another person may sign if directed | If the maker cannot physically sign, someone else may sign for them in their presence and by their direction. | true | Record who signed, why, and that they signed by the maker's direction and in the maker's presence. |
Capacity | |||
Communication support should be used where needed | A person is not unable to decide merely because they communicate differently. | false | Use interpreters, communication aids or supported decision-making and note the support used. |
Capacity should be presumed unless shown otherwise | Adults are presumed to have capacity unless there is evidence they lack it. | false | Do not assume incapacity because of age, disability, illness or an unwise decision. |
An unwise refusal does not prove lack of capacity | A person can make a decision others think unwise and still have capacity. | true | Record that risks and consequences were understood when the decision was made. |
Decision should be free from pressure | Coercion or undue influence may cast doubt on whether the refusal truly reflects the maker's decision. | true | Discuss serious refusals privately with a clinician or adviser and record that the decision was voluntary. |
Review | |||
Complex refusals should be discussed with a clinician | Clinical input helps make treatment names, consequences and circumstances accurate. | true | Ask your GP, consultant or palliative care team to review the wording. |
Communication | |||
Care providers should hold a copy | Care homes and hospitals often need quick access during deterioration or transfer. | true | Ask the care home and hospital team to add it to care records and handover notes. |
Emergency services should be alerted if relevant | Emergency clinicians may need immediate evidence before withholding life-sustaining treatment. | true | Ask your GP or care team about local emergency care records, DNACPR forms or alert systems. |
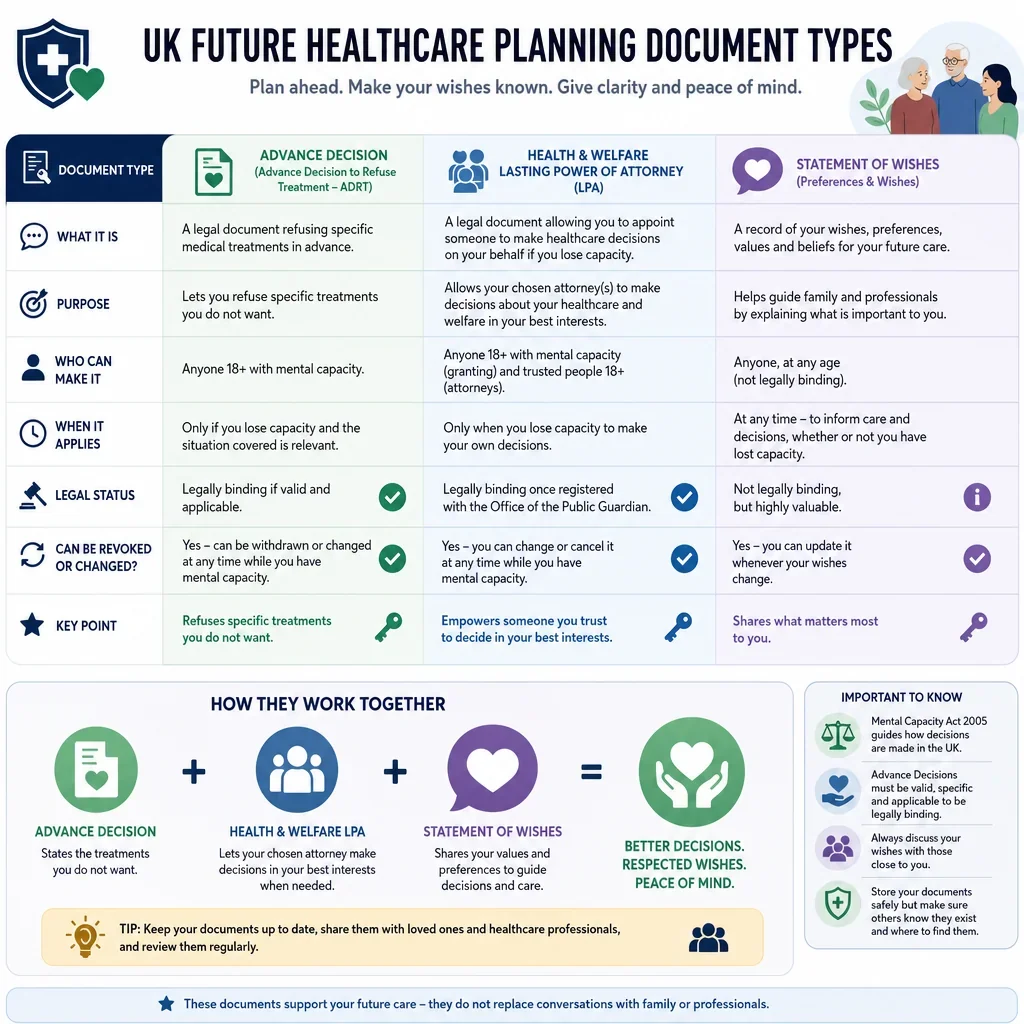
Advance statements are not the same as refusals | An advance statement expresses wishes and preferences an Advance Decision refuses specified treatment. | false | Keep refusal clauses separate from wider care preferences. |
Legal validity | |||
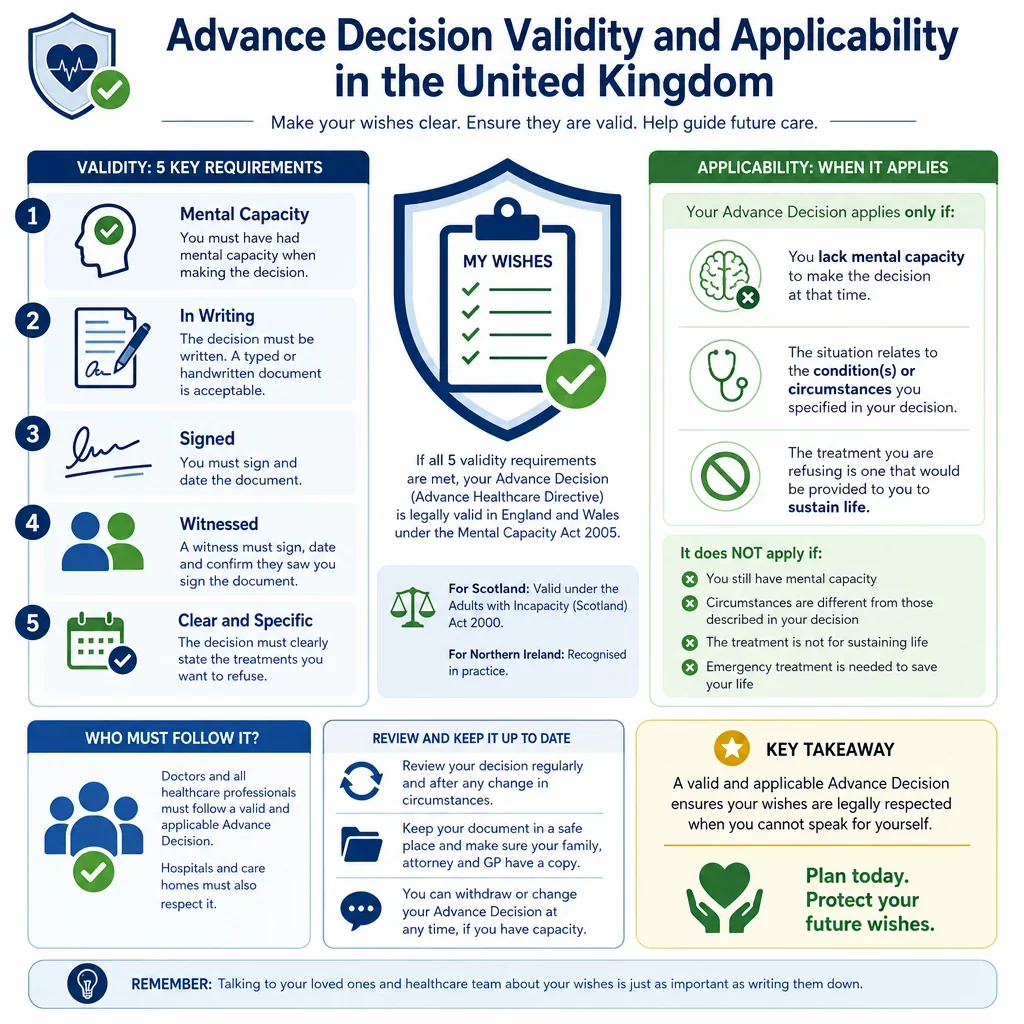
England and Wales law should be identified | The Mental Capacity Act 2005 rules apply in England and Wales other UK nations have different frameworks. | false | State the document is intended for use in England and Wales and seek local advice if moving within the UK. |
Scotland uses different legal terminology | Scottish incapacity law differs from the Mental Capacity Act 2005 framework. | false | Take Scottish legal or clinical advice if the document may be used in Scotland. |
Northern Ireland has a different capacity framework | Rules and terminology for future healthcare decisions may differ in Northern Ireland. | false | Get Northern Ireland-specific advice if treatment may occur there. |
Communication | |||
Document should be legible and accessible | Illegible or inaccessible documents are harder to rely on in urgent care. | true | Keep a clean signed copy, digital scan and clear note of where the original is held. |
Legal validity | |||
Document should not contain conflicting instructions | Contradictions can make it unclear whether the refusal applies. | true | Check that refusals, exceptions, advance statements and LPA wording align. |
Communication | |||
Information sharing consent may help | Clear permission can make it easier for clinicians to discuss the document with named contacts. | false | Name who may be contacted about the document and add their phone numbers. |
Maker must be clearly identified | Clinicians must be sure the document belongs to the patient being treated. | true | Include full name, date of birth, NHS number if known, address and previous names. |
Applicability | |||
Exceptions should be tightly drafted | Unclear exceptions can make it difficult to decide whether treatment is refused. | true | State exactly when a refused treatment may still be given, if any exception is intended. |
Communication | |||
Palliative care wishes should be separated from refusals | Comfort care preferences guide care but are not usually treatment refusals. | false | Use a separate section for pain relief, place of care, spiritual needs and family contact. |
Review | |||
Reviews should be documented | A dated review note helps show the maker still intended the refusal to stand. | true | Add a signed and dated review statement, or execute a fresh version after major changes. |
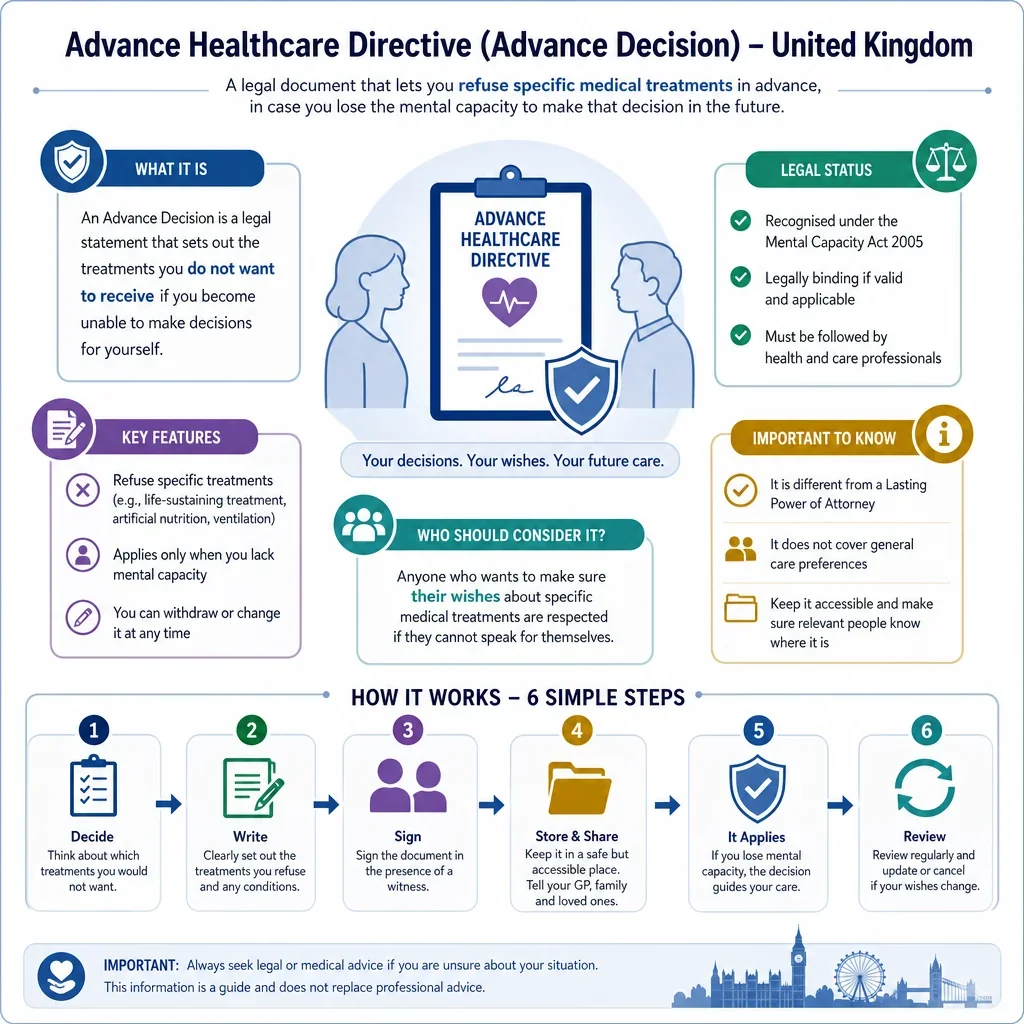
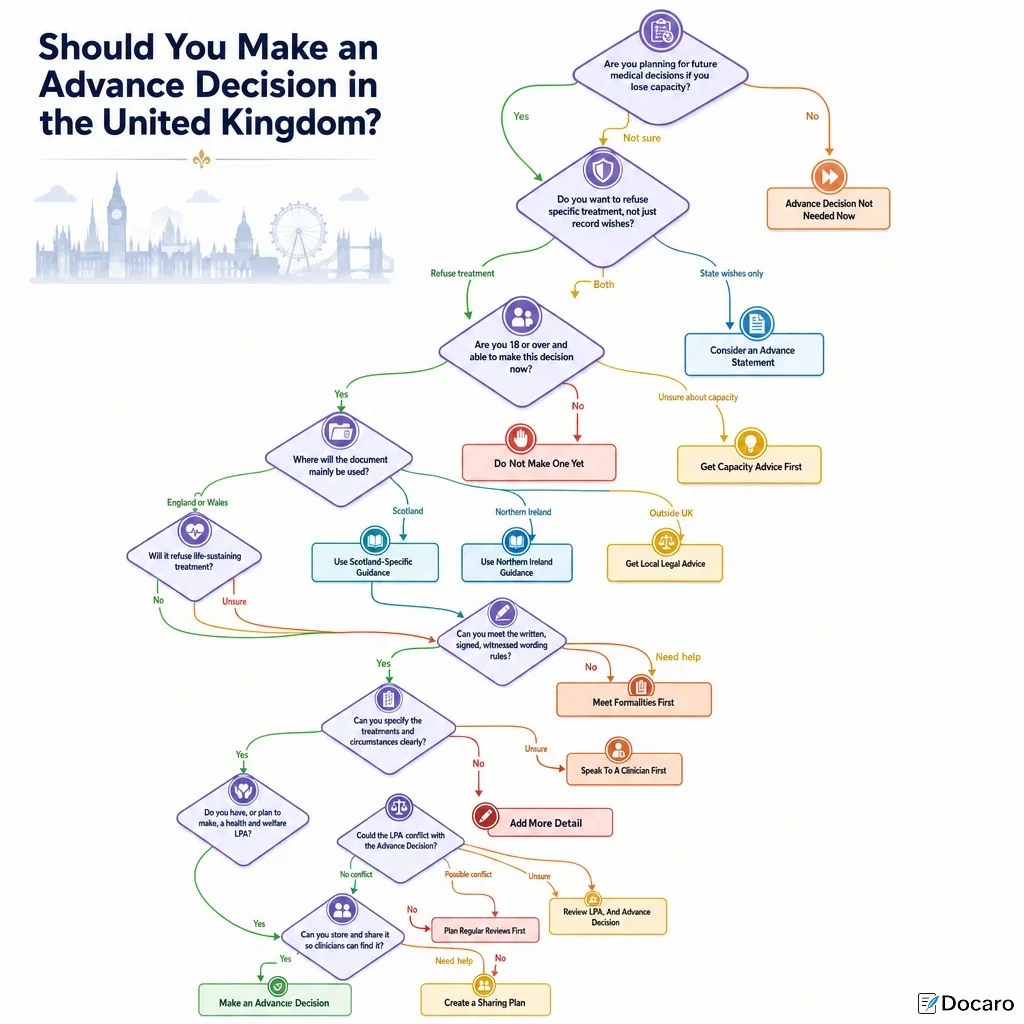
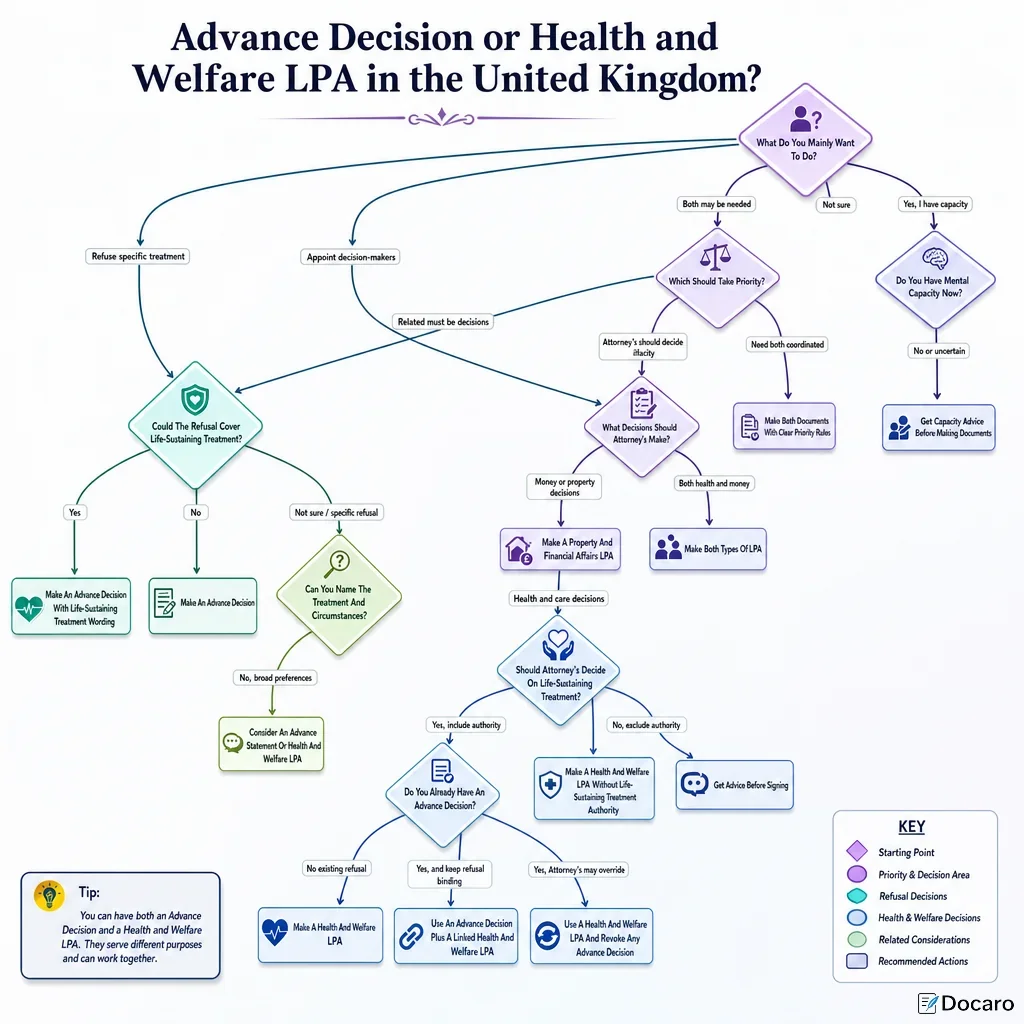
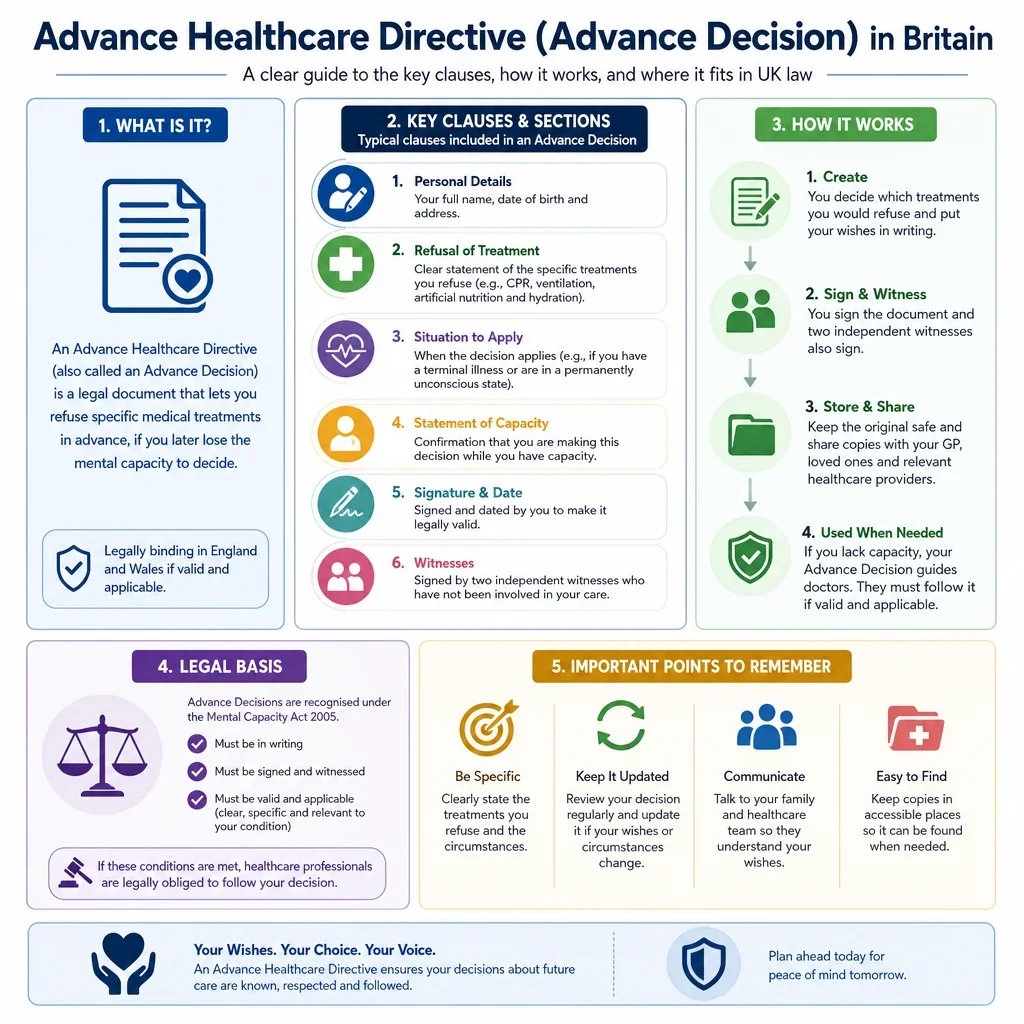
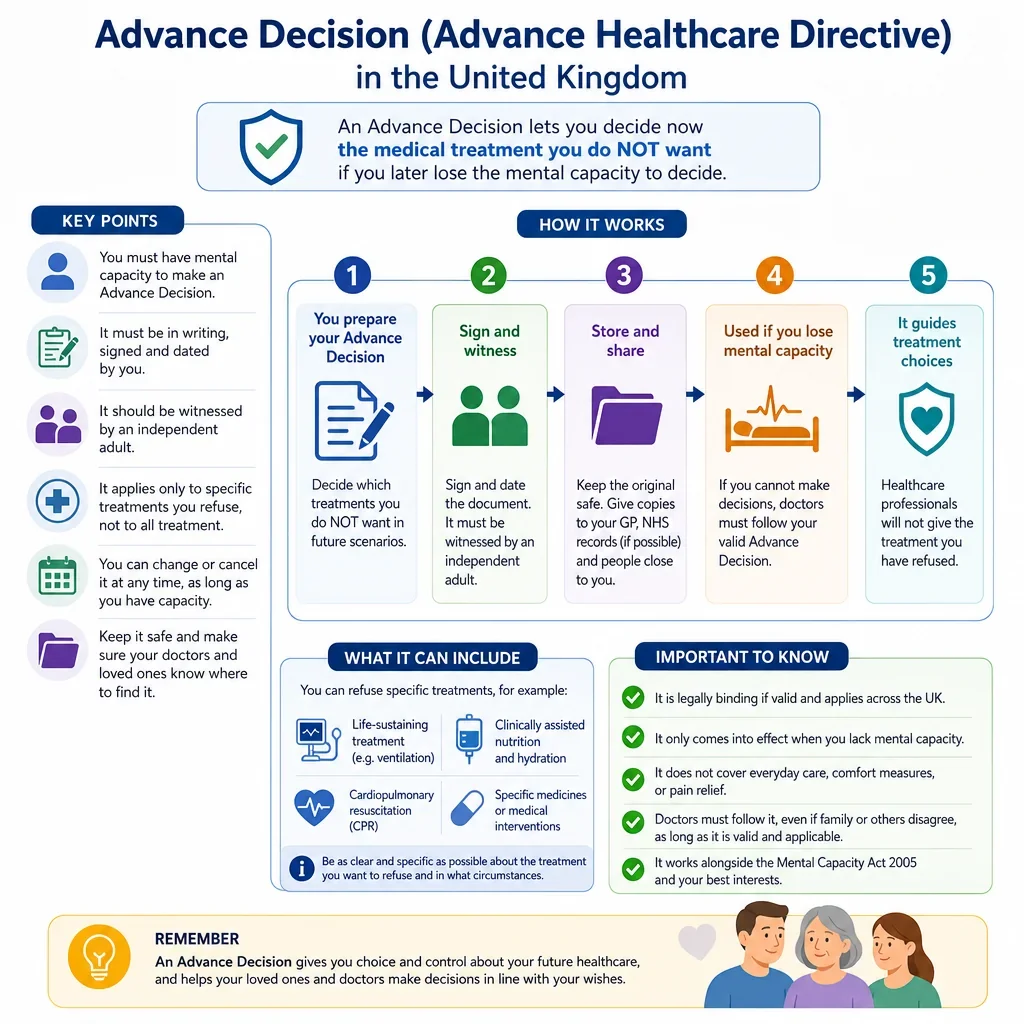
How Do You Make An Advance Decision Valid In England And Wales?
An Advance Decision must be made by a person aged 18 or over who has capacity at the time, and it must clearly identify the treatment being refused and the circumstances in which the refusal applies. For refusals of life-sustaining treatment, extra formalities apply: it must be in writing, signed by the maker or someone signing on their behalf, witnessed, and include a clear statement that the refusal applies even if life is at risk.
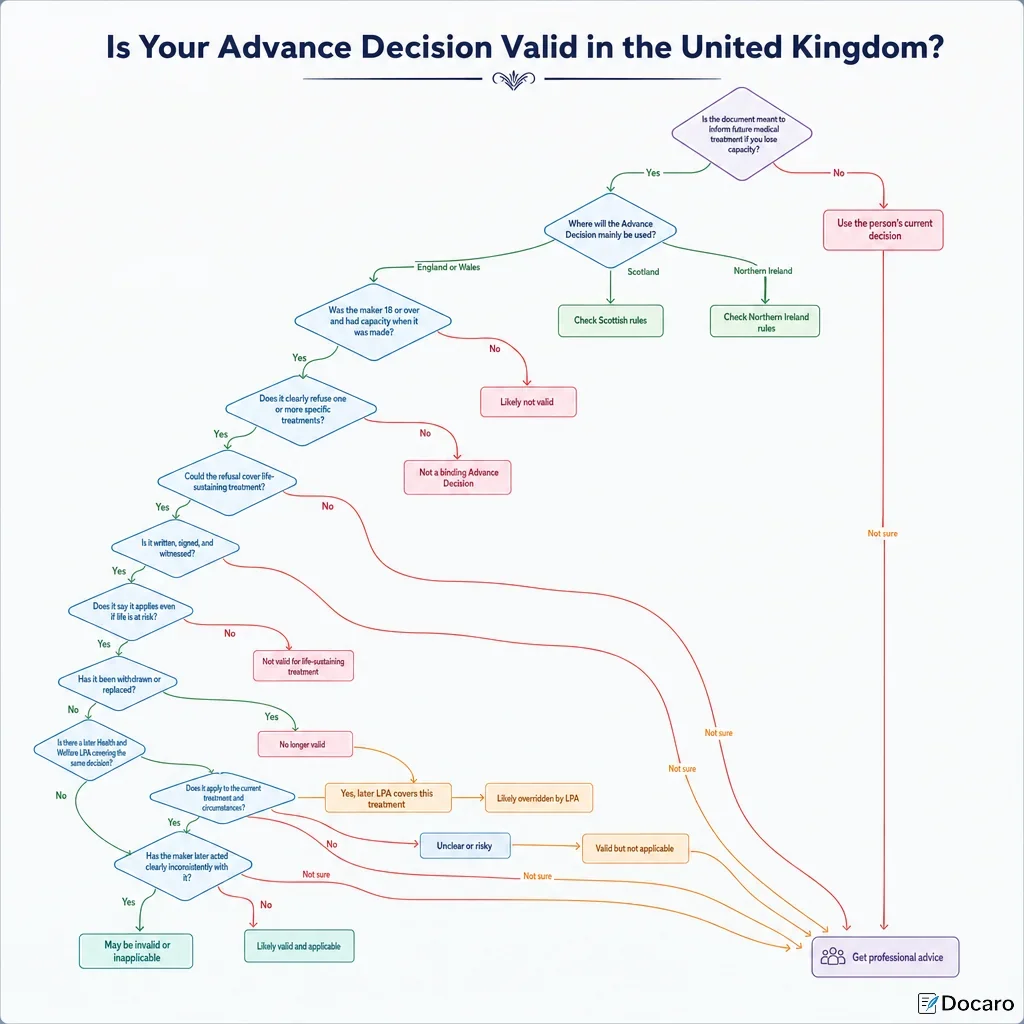
When Will Doctors Follow An Advance Decision?
Doctors must consider whether the Advance Decision is both valid and applicable to the current treatment and circumstances. It may not be followed if the person has withdrawn it, later made a conflicting Lasting Power of Attorney for health and welfare, acted inconsistently with it, or the current situation was not anticipated when it was made.
What Practical Steps Reduce The Risk Of Disputes?
- Use precise wording for the treatment refused and the medical situations covered.
- Add the statutory life-sustaining treatment wording if relevant.
- Sign and witness the document correctly.
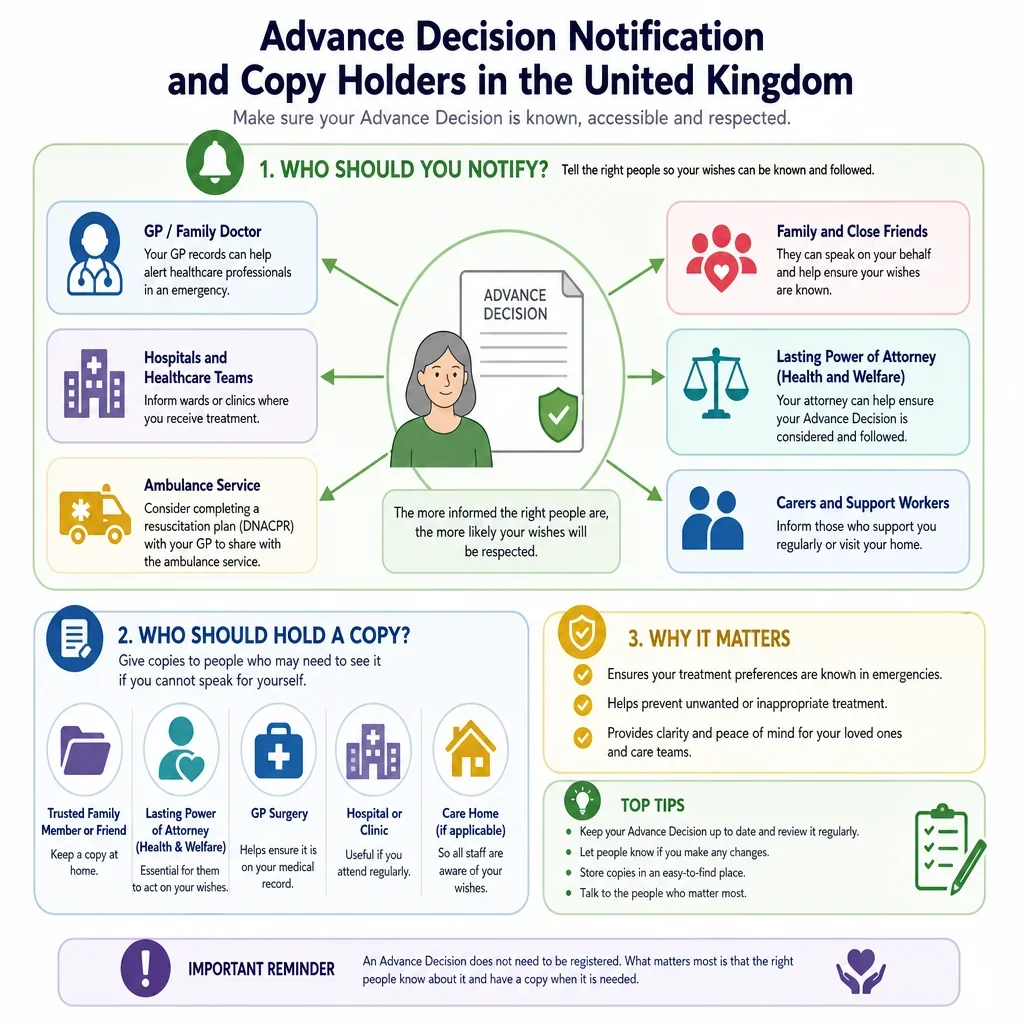
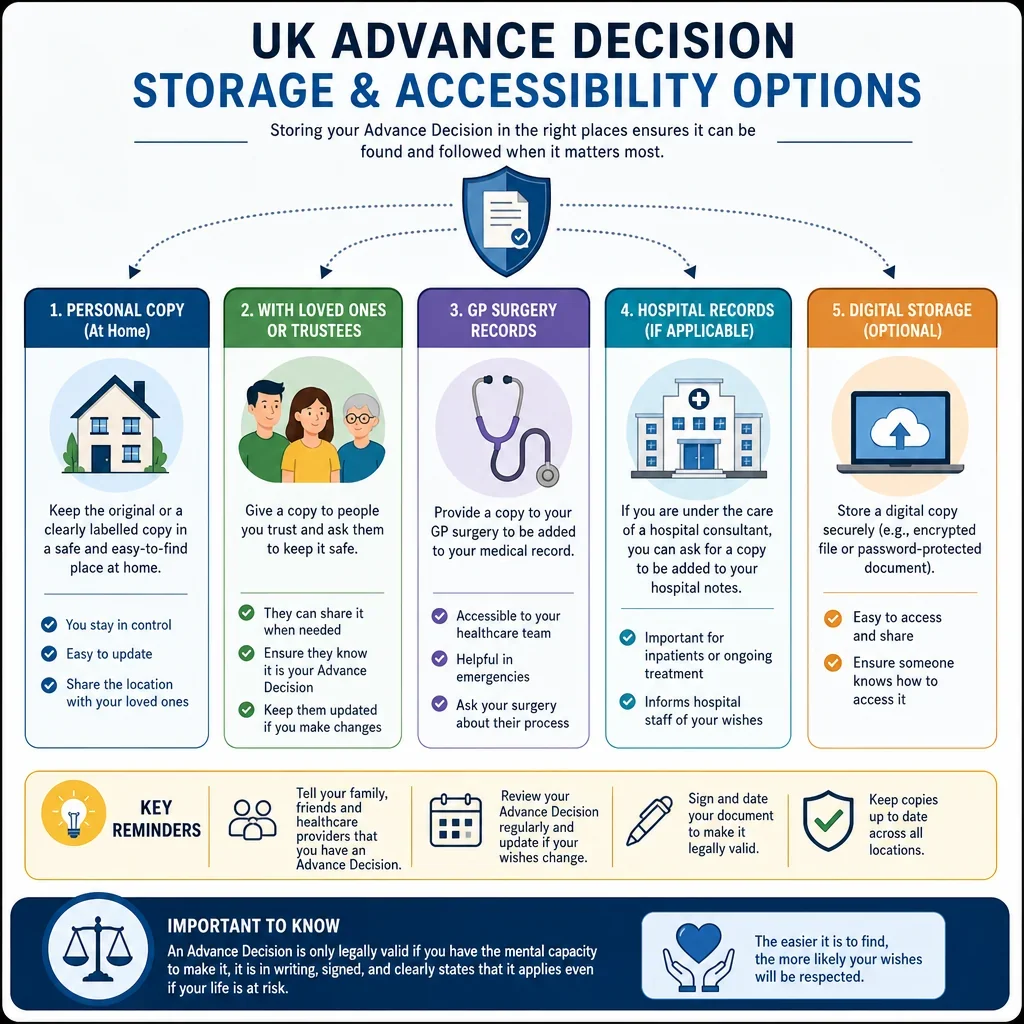
- Tell your GP, hospital team, attorney and close family where the document is kept.
- Review it after any major diagnosis, change in treatment options, or change in personal wishes.
FAQs
You Might Also Be Interested In